

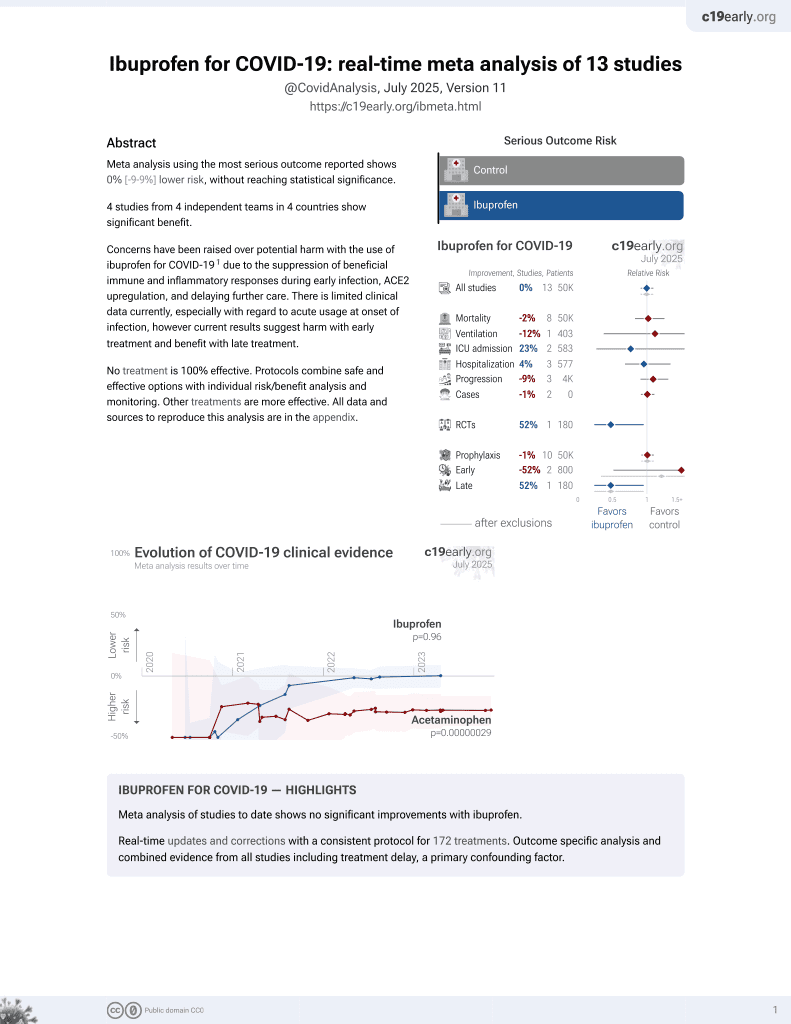
Ibuprofen for COVID-19: real-time meta analysis of 13 studies
 Control
ControlAbstract
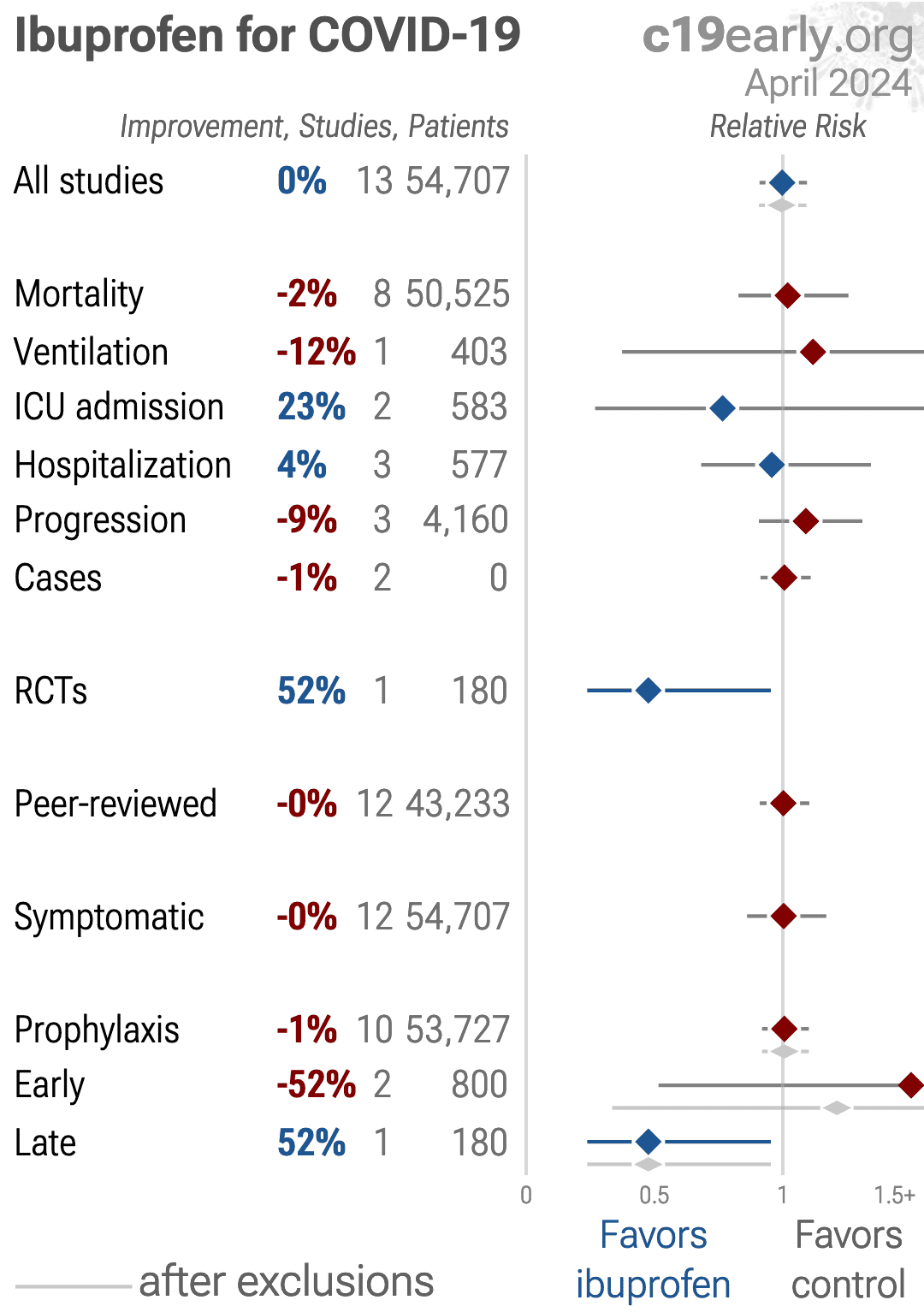
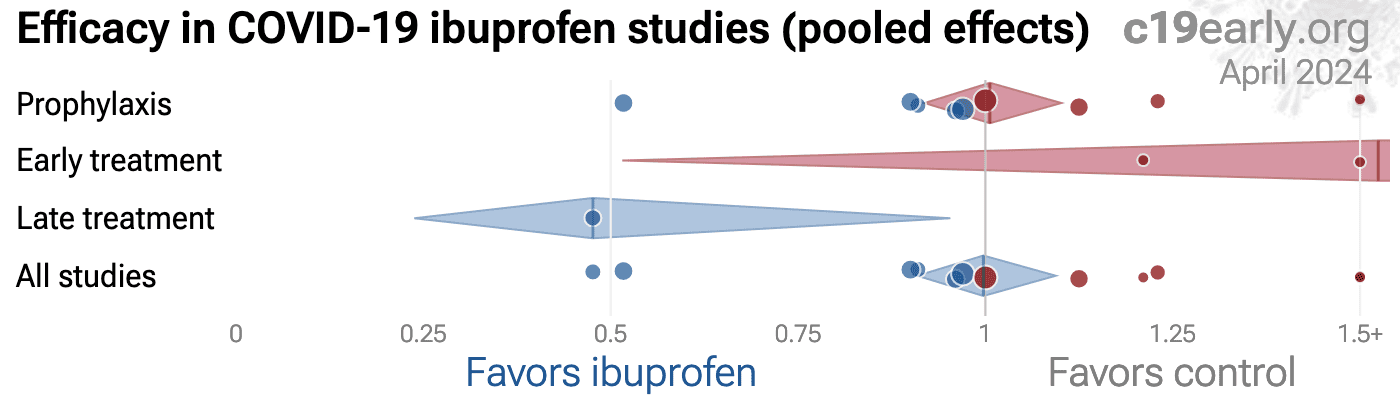
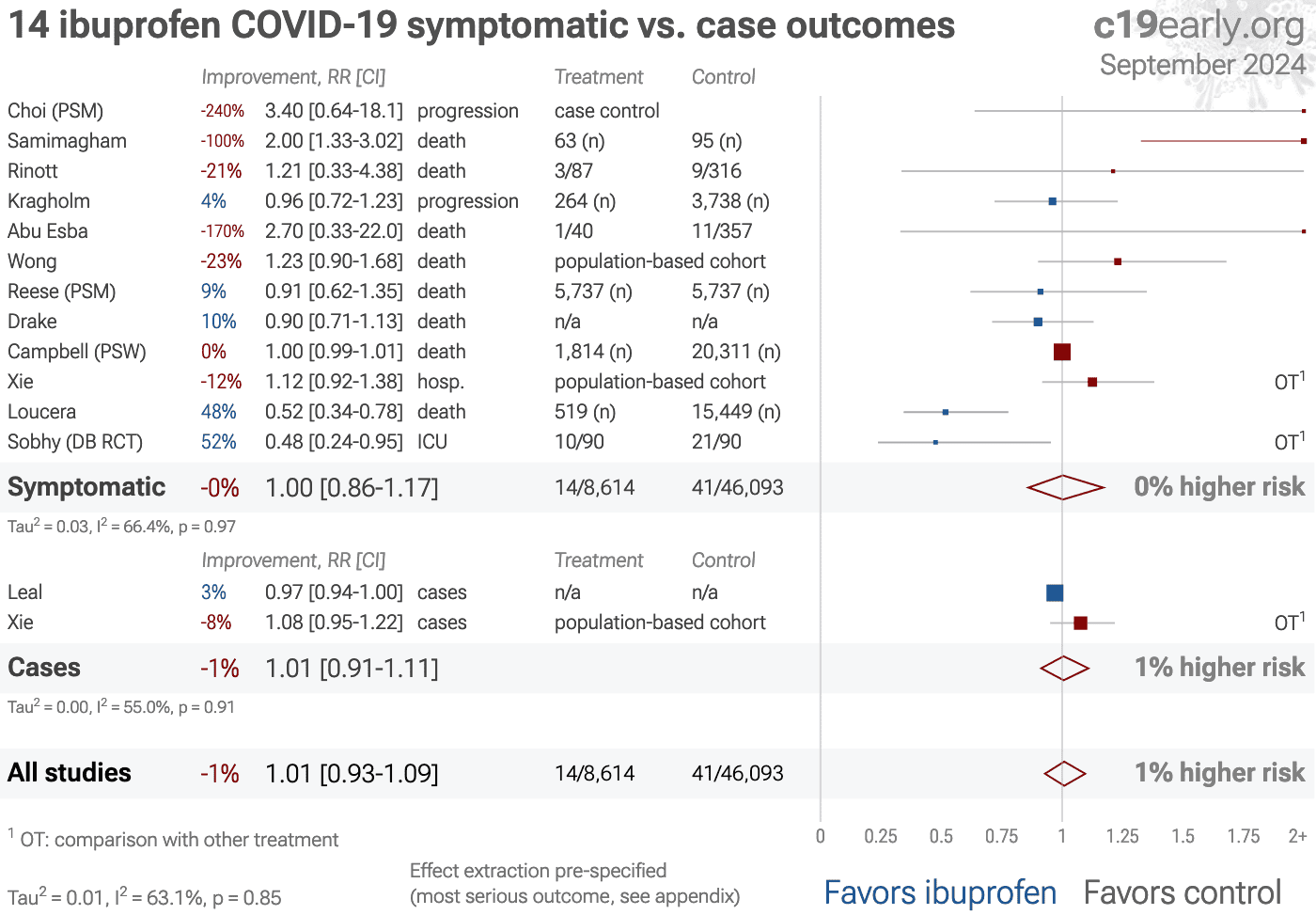
Meta analysis using the most serious outcome reported shows
0% [-9‑9%] lower risk, without reaching statistical significance.
4 studies from 4 independent teams in 4 countries show significant
benefit.
Concerns have been raised over potential harm with the use of ibuprofen for COVID-191 due to the suppression of beneficial immune and inflammatory responses during early infection, ACE2 upregulation, and delaying further care. There is limited clinical data currently, especially with regard to acute usage at onset of infection, however current results suggest harm with early treatment and benefit with late treatment.
No treatment is 100%
effective. Protocols combine safe and effective options with individual
risk/benefit analysis and monitoring.
Other treatments are more effective.
All data and sources to reproduce this analysis are in the appendix.
Ibuprofen for COVID-19 — Highlights
Meta analysis of studies to date shows no significant improvements with ibuprofen.
Real-time updates and corrections with a consistent protocol for 172 treatments. Outcome specific analysis and combined evidence from all studies including treatment delay, a primary confounding factor.
B
Loading..
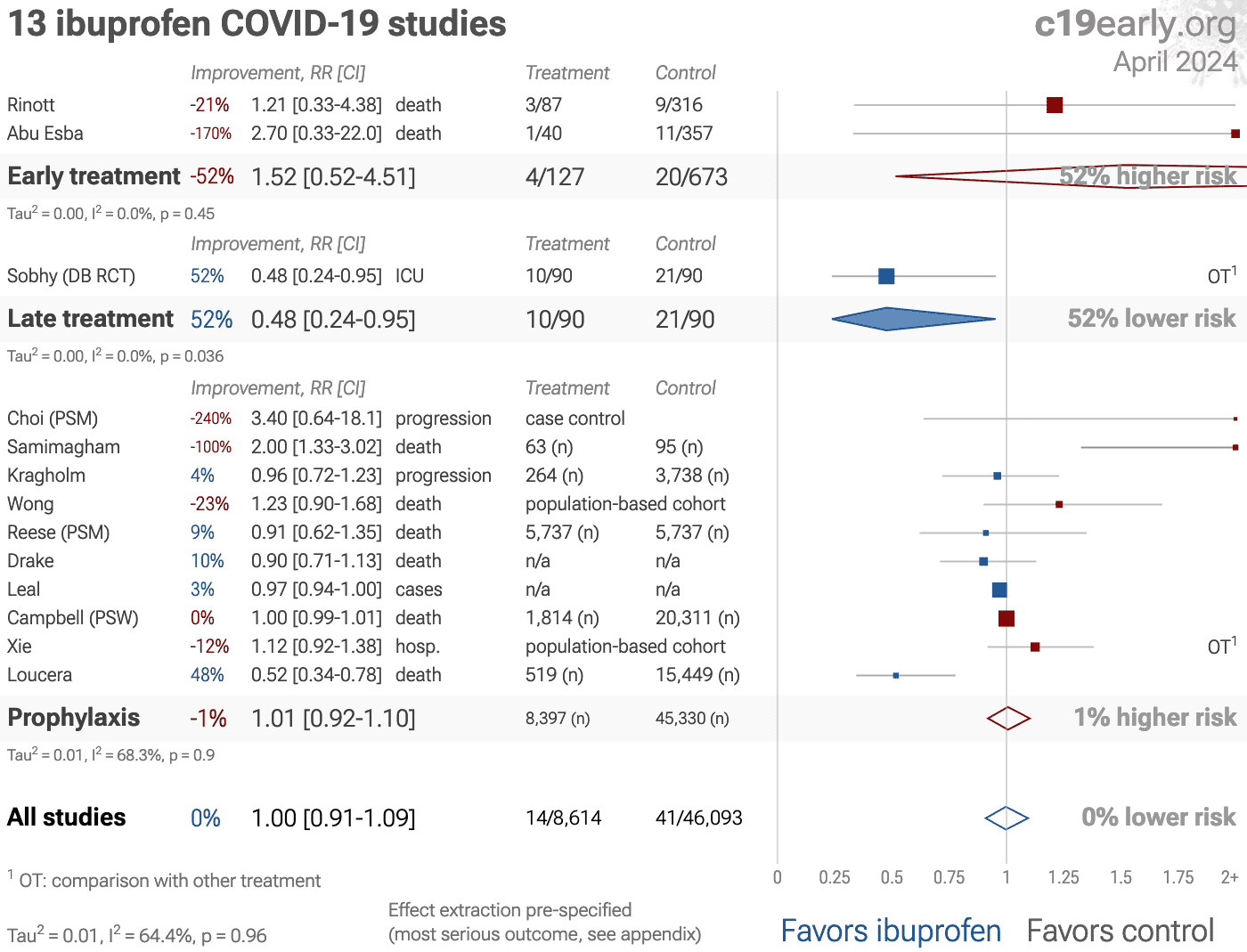
Figure 1. A. Random effects meta-analysis. This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
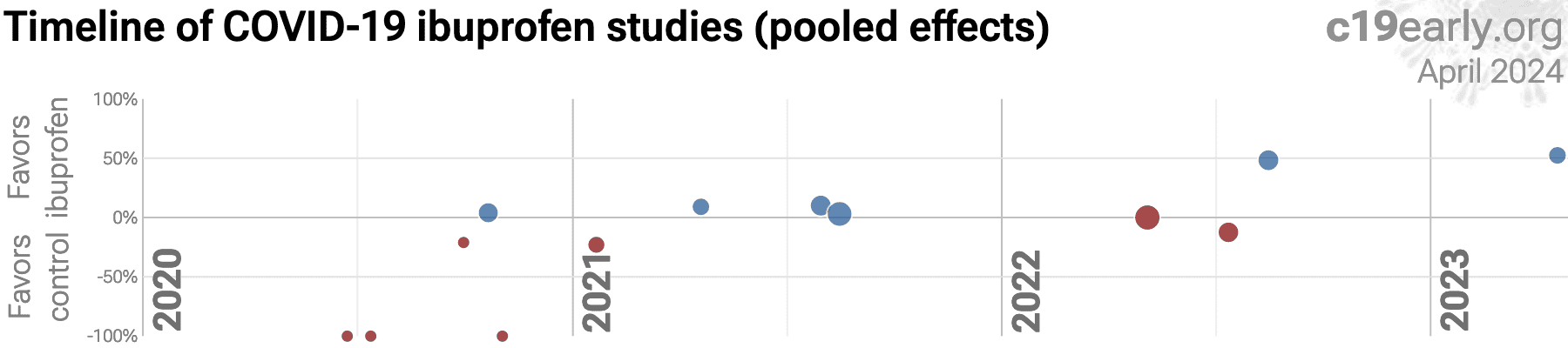
B. Timeline of results in ibuprofen studies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
SARS-CoV-2 infection primarily begins in the upper respiratory
tract and may progress to the lower respiratory tract, other tissues, and the
nervous and cardiovascular systems, which may lead to cytokine storm,
pneumonia, ARDS, neurological injury3-15 and
cognitive deficits6,11, cardiovascular
complications16-20, organ failure, and death.
Even mild untreated infections may result in persistent cognitive
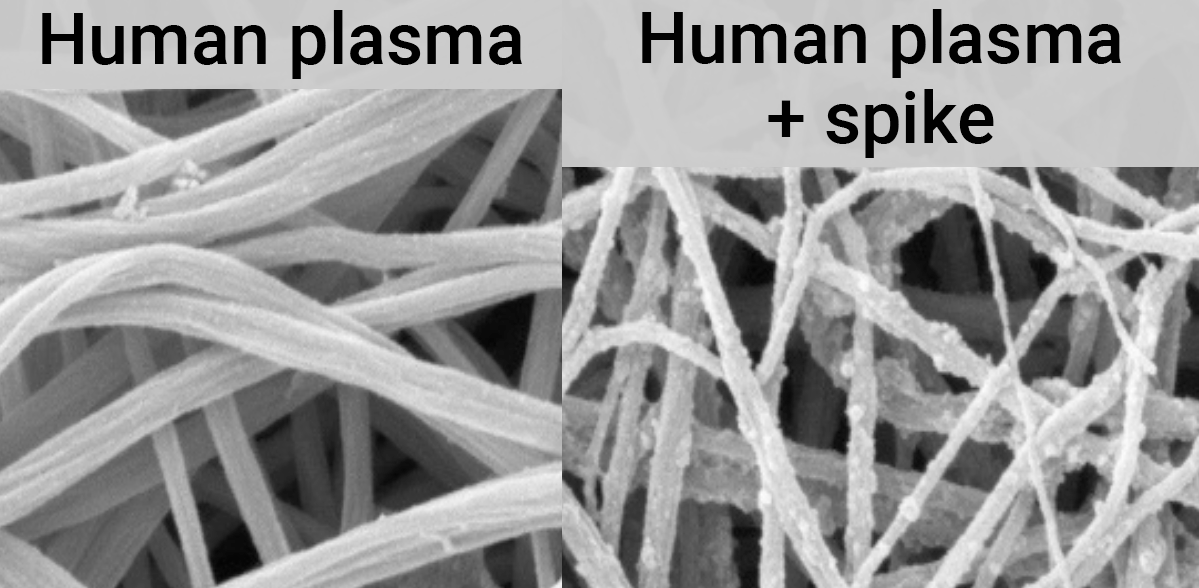
deficits21—the spike protein binds to fibrin leading to
fibrinolysis-resistant blood clots, thromboinflammation, and
neuropathology.
Minimizing replication as early as possible is recommended.
SARS-CoV-2 infection and replication involves the complex interplay of 100+
host and viral proteins and other factorsA,22-29, providing many
therapeutic targets for which many existing compounds have known activity.
Scientists have predicted that over 9,000 compounds may
reduce COVID-19 risk30, either by
directly minimizing infection or replication, by supporting immune system
function, or by minimizing secondary complications.
We analyze all significant
controlled studies of
ibuprofen
for COVID-19.
Search methods, inclusion criteria, effect extraction criteria (more serious
outcomes have priority), all individual study data, PRISMA answers, and
statistical methods are detailed in Appendix 1. We present random
effects meta-analysis results for all studies, studies within each treatment stage, individual outcomes, peer-reviewed studies, Randomized Controlled Trials (RCTs), and higher quality studies.
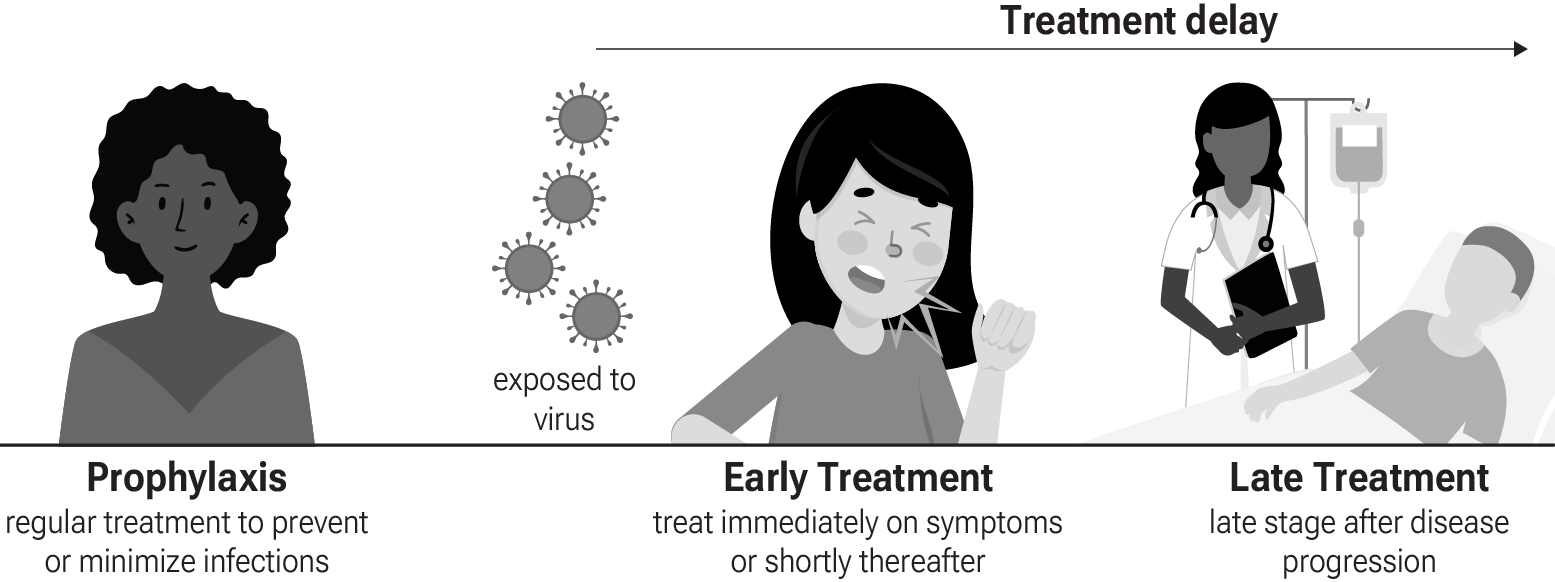
Figure 3 shows stages of possible treatment for
COVID-19. Prophylaxis refers to regularly taking medication before
becoming sick, in order to prevent or minimize infection. Early
Treatment refers to treatment immediately or soon after symptoms appear,
while Late Treatment refers to more delayed treatment.
{kind=link}
Figure 3. Treatment stages.
Stuart et al. performed a retrospective study of 142,925
outpatients in the UK showing significantly higher risk of hospitalization or
death with prescription of NSAIDs for respiratory tract infections, OR 3.19
[2.42-4.23]. Practice-level analysis also found a 0.32 percentage point
increase in hospitalizations/deaths for every 1 percentage point increase in
NSAID prescribing, which increases confidence in an assocation rather than
confounding by indication.
NSAIDs may be harmful due to suppression of inflammatory and
immune responses needed to clear infections. They inhibit cyclooxygenase
enzymes and production of prostaglandins involved in inflammation. This
anti-inflammatory effect could hamper the body's ability to fight the
infection. NSAIDs may mask symptoms of worsening infection. By reducing pain,
fever, and inflammation, they could provide symptomatic relief while the
infection progresses unchecked, delaying further medical care. NSAIDs may
increase risks of certain complications, for example some evidence links
NSAIDs to a higher risk of cardiovascular events.
For COVID-19, the potential harm or benefit may depend strongly
on the timing of use, and any direct antiviral effects of the specific NSAID.
For example, anti-inflammatory effects may be detrimental at the early stage
of COVID-19 infection, but may be helpful in later stages depending on
severity.
While there is very limited evidence to date, notably current results
for ibuprofen suggest harm with early treatment and benefit with late
treatment.
Fever is an important component of the acute response to coronavirus
infection32.
The evolutionary conservation of fever for over 600 million years supports
a survival benefit33.
Viral particle sensing occurs via pattern recognition receptors, such as toll-like
receptors, triggering release of endogenous pyrogens such as interleukin-1.
These cytokines induce thermoregulatory centers in the hypothalamus to elevate
core temperature setpoints above normal homeostasis. The resulting fever
enhances multiple aspects of the innate and adaptive immune systems33,
and creates a suboptimal internal
environment that impairs SARS-CoV-2 enzyme function and replication.
In Vitro studies demonstrate reduced viral output at sustained febrile
temperatures of 38-39°C compared to basal 37°C conditions. Fever also
correlates clinically with heightened interferon-γ, interleukin-6, lymphocyte
activation, and antibody production critical for viral clearance.
Los et al. showed that higher temperature enhanced the expression of
antiviral genes and reduced SARS-CoV-2 replication in Calu-3 and Caco-2 cells.
An in vivo hamster model showed that higher body temperature at the time of
infection correlated with lower viral loads.
Zhou et al. showed that SARS-CoV-2 patients with higher fever had lower viral load.
Molecular dynamics simulations, surface plasmon resonance experiments, and pseudovirus cell entry assays showed decreased SARS-CoV-2 binding affinity to the human ACE2 receptor at higher temperature (40°C vs. 37°C).
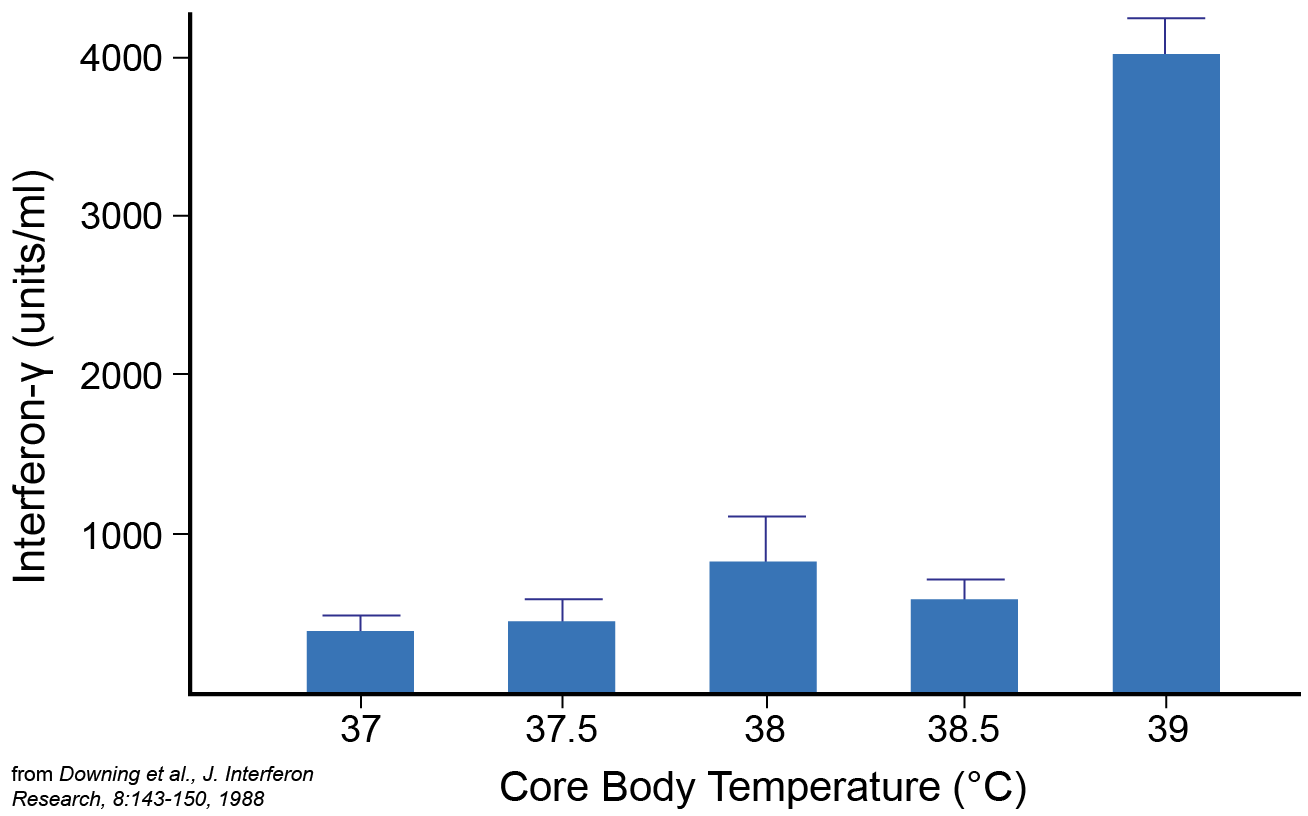
Downing et al. induced hyperthermia (fever-like
temperatures) in human volunteers by immersing them in warm water baths. They
found that lymphocytes isolated from individuals with core body temperatures
elevated to 39°C produced up to 10 times more interferon-γ, as shown in
Figure 4. They also found an increase in suppressor/cytotoxic T
cells and natural killer cells. The threshold of 39°C suggests relevance to
fever, and the results suggest fever may play a role in boosting antiviral and
immunoregulatory activities.
{kind=link}
Figure 4.
A 10 fold increase in interferon-γ production was seen
when core body temperature reached 39°C, from Downing et al.
Herder et al. perform in vitro analysis with a 3D
respiratory epithelial model using cells from human donors. Authors showed
that elevated temperature (39-40°C) restricts SARS-CoV-2 infection and
replication independently of interferon-mediated antiviral defenses. Authors
found SARS-CoV-2 can still enter respiratory cells at 40°C but viral
transcription and replication are inhibited, limiting the production of
infectious virus. This temperature-dependent restriction correlates with
altered host gene expression related to antiviral immunity and epigenetic
regulation. The results suggest that febrile temperature ranges may confer
protection to respiratory tissues by restricting SARS-CoV-2 propagation.
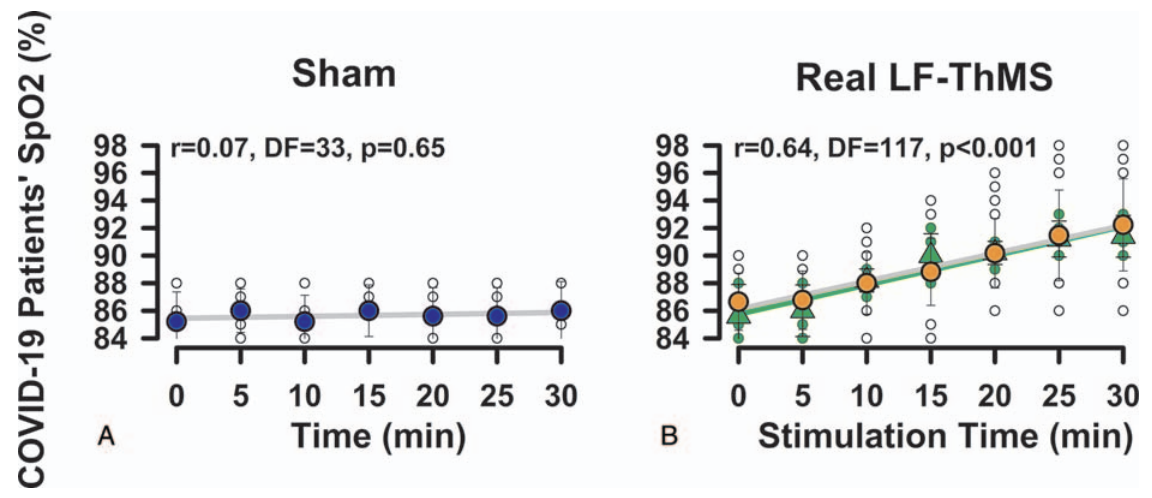
Dominguez-Nicolas et al. induced localized hyperthermia
using LF-ThMS applied to the dorsal thorax (up to 44°C externally), resulting
in significantly increased peripheral oxygen saturation (SpO2)
levels in COVID-19 patients, as shown in Figure 5.
{kind=link}

Figure 5.
Rapidly increasing SpO2 in COVID-19 patients with localized thoracic hyperthermia, from Dominguez-Nicolas et al.
Ramirez et al. compared COVID-19 mortality in Finland and
Estonia, where sauna use is part of the culture and is typically practiced at
least once a week, with the rest of Europe. Authors found significantly lower
mortality with sauna culture, and suggest this may be due to the beneficial
effects of hydrothermotherapy.
Ruble et al. compared army hospital vs. sanitarium
treatment for the 1918 Spanish influenza, showing lower progression to
pneumonia and lower mortality with sanitarium treatment, which involves
hydrothermotherapy, sunlight, and fresh air.
Stewart reports on the use of diathermy in the treatment of
pneumonia in 1926, with case reports from several physicians covering over 300
patients. Author reports that diathermy had consistent positive effects
without significant adverse events, resulted in about half the mortality of
the control group, significantly alleviated symptoms such as dyspnea, pain,
and cardiac strain, and improved sleep and reduced respiratory rates.
Recent atom-level work strengthens the mechanistic case for fever-mediated viral
attenuation. Xie et al. performed 200-ns equilibration followed by replicate 100-ns
all-atom MD simulations of the spike RBD–ACE2 peptidase complex across physiologic-to-febrile
temperatures. At 315 K the interface lost ~1 hydrogen bond, solvent exposure grew by ~4 Ų,
dissociation probability tripled, and MM-PBSA binding free energy became ≈59 kcal mol-¹ less
favorable, driven by heat-induced straightening of the ACE2 α1-helix and withdrawal of
the β3β4 hairpin that jointly destabilise the two anchor regions. Mild-cool conditions (305 K)
had the opposite effect, α1-helix curvature tightened the interface, dissociation dropped eight-fold, and binding free energy became ~21 kcal mol-¹ more favorable. These thermodynamic
shifts directly support febrile-range hyperthermia as a barrier to initial viral attachment.
In summary, fever is a key component of the response to
infection. Fever enhances immune cell performance, induces cellular stress on
pathogens, and may act synergistically with other stressors like iron
deprivation. While results show beneficial effects of fever, it is not
universally beneficial. Extreme or prolonged cases may be harmful. Fever may
be more detrimental for individuals with lower tolerance for the increased
metabolic demands.
Fever may also reduce transmissibility. Fever helps clear
infection faster by enhancing immune responses and applying cellular stress to
pathogens. Faster clearance gives the pathogen less time to amplify within the
host to reach contagious levels. Fever may also apply evolutionary pressure
resulting in sacrificing replicative fitness at normal temperatures,
minimizing infection in other hosts. Further, fever promotes reduced activity,
minimizing the opportunity for transmission.
The beneficial effects of fever suggest potential harm from
fever-reducing medications in terms of an increased risk of poor outcomes and
increased transmission. However, these may be offset by other effects of specific
medications, including anticoagulant, anti-inflammatory, or antiviral effects.
Notably, studies for COVID-19 show significantly increased risk with
acetaminophen43.
Table 1 summarizes the results for all stages combined, for Randomized Controlled Trials, for peer-reviewed studies, after exclusions, and for specific outcomes.
Table 2 shows results by treatment stage.
Figure 6 plots individual results by treatment stage.
Figure 7, 8, 9, 10, 11, 12, 13, 14, 15, and 16
show forest plots for random effects meta-analysis of
all studies with pooled effects, mortality results, ventilation, ICU admission, hospitalization, progression, recovery, cases, peer reviewed studies, and non-symptomatic vs. symptomatic results.
| Relative Risk | Studies | Patients | |
|---|---|---|---|
| All studies | 1.00 [0.91‑1.09] | 13 | 50K |
| After exclusions | 1.00 [0.91‑1.09] | 12 | 50K |
| Peer-reviewedPeer-reviewed | 1.00 [0.91‑1.10] | 12 | 40K |
| RCTsRCTs | 0.48 [0.24‑0.95]* | 1 | 180 |
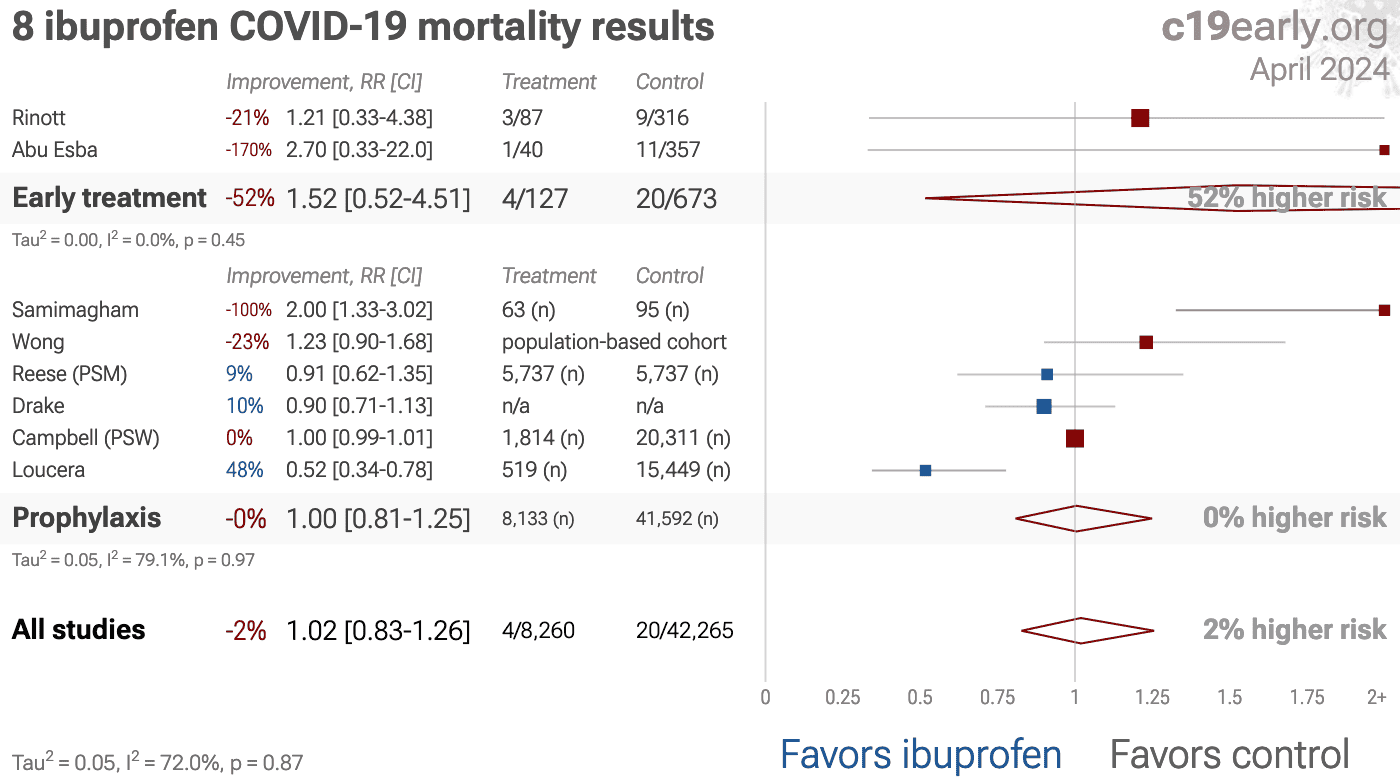
| Mortality | 1.02 [0.83‑1.26] | 8 | 50K |
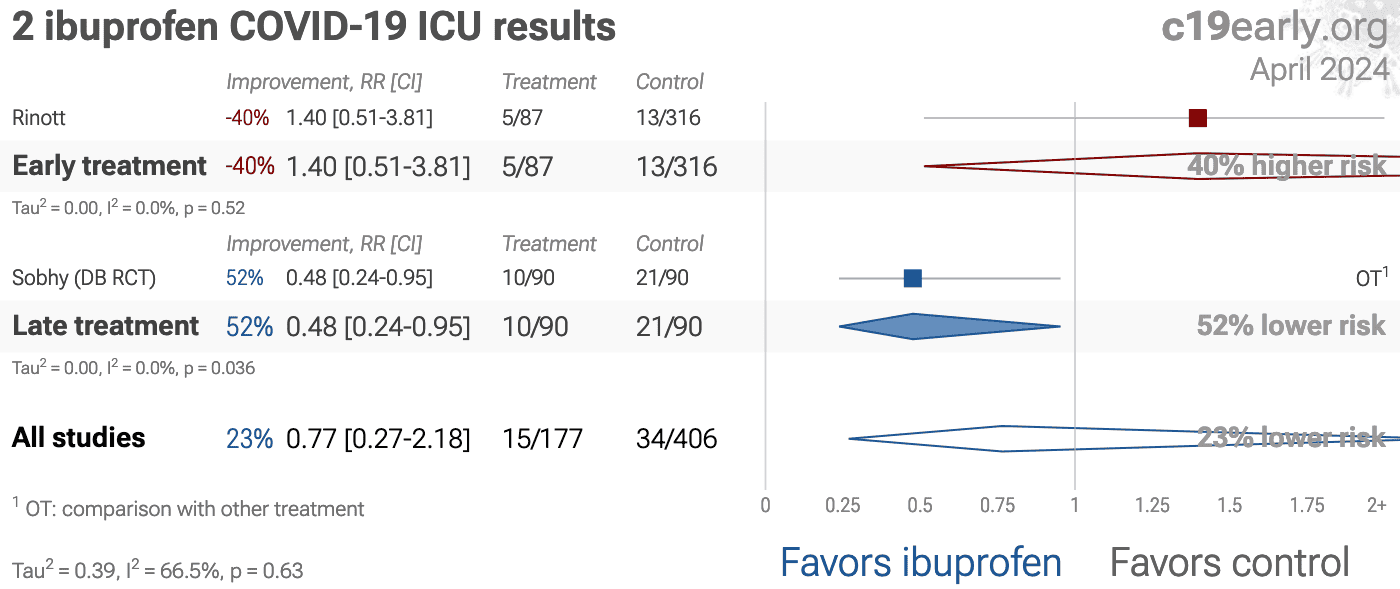
| ICU admissionICU | 0.77 [0.27‑2.18] | 2 | 583 |
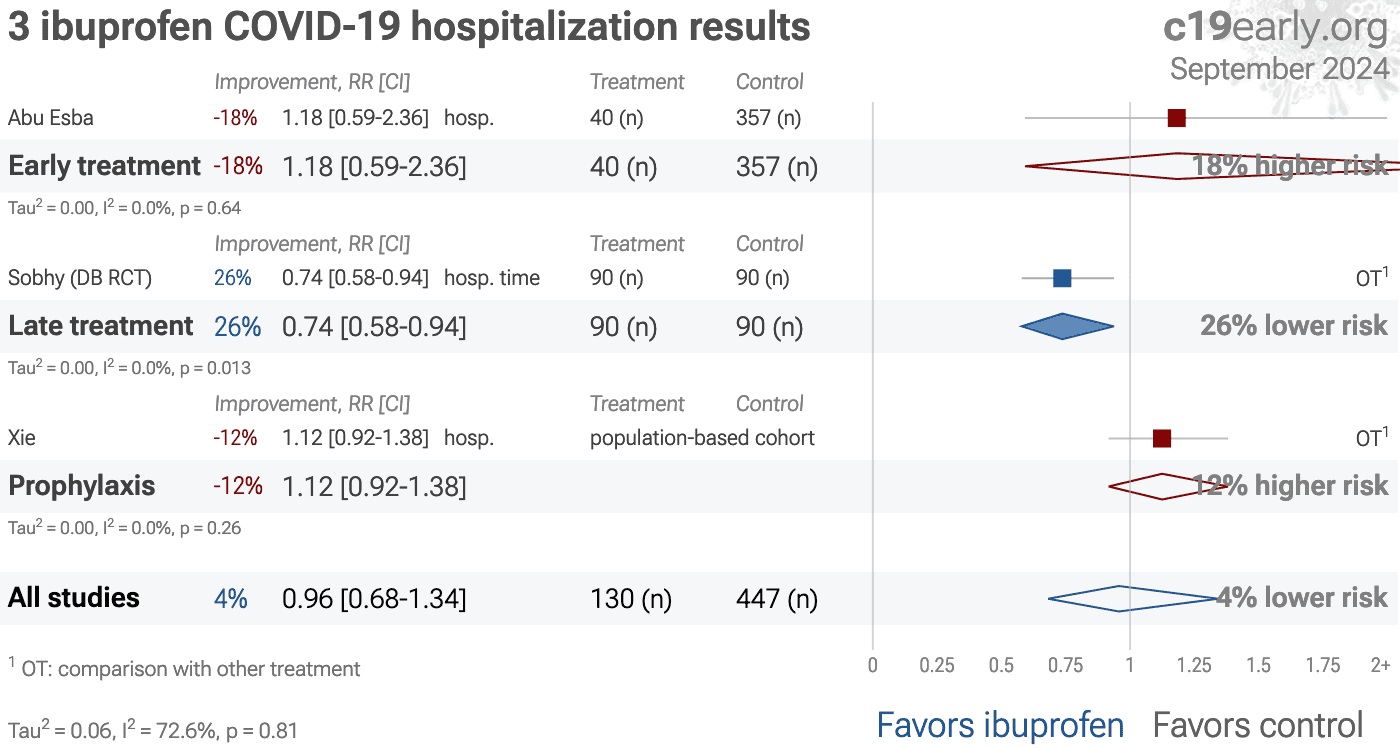
| HospitalizationHosp. | 0.96 [0.68‑1.34] | 3 | 577 |
| Cases | 1.01 [0.91‑1.11] | 2 | 0 |
| Early treatment | Late treatment | Prophylaxis | |
|---|---|---|---|
| All studies | 1.52 [0.52‑4.51]1.52 [0.52‑4.51] | 0.48 [0.24‑0.95]*0.48* [0.24‑0.95] | 1.01 [0.92‑1.10]1.01 [0.92‑1.10] |
| After exclusions | 1.21 [0.33‑4.38]1.21 [0.33‑4.38] | 0.48 [0.24‑0.95]*0.48* [0.24‑0.95] | 1.01 [0.92‑1.10]1.01 [0.92‑1.10] |
| Peer-reviewedPeer-reviewed | 1.52 [0.52‑4.51]1.52 [0.52‑4.51] | 0.48 [0.24‑0.95]*0.48* [0.24‑0.95] | 1.01 [0.92‑1.11]1.01 [0.92‑1.11] |
| RCTsRCTs | 0.48 [0.24‑0.95]*0.48* [0.24‑0.95] | ||
| Mortality | 1.52 [0.52‑4.51]1.52 [0.52‑4.51] | 1.00 [0.81‑1.25]1.00 [0.81‑1.25] |
|
| ICU admissionICU | 1.40 [0.51‑3.81]1.40 [0.51‑3.81] | 0.48 [0.24‑0.95]*0.48* [0.24‑0.95] | |
| HospitalizationHosp. | 1.18 [0.59‑2.36]1.18 [0.59‑2.36] | 0.74 [0.58‑0.94]*0.74* [0.58‑0.94] | 1.12 [0.92‑1.38]1.12 [0.92‑1.38] |
| Cases | 1.01 [0.91‑1.11]1.01 [0.91‑1.11] |
||
{kind=link}
Figure 6. Scatter plot showing the most serious outcome in all studies, and for studies within each stage. Diamonds shows the results of random effects meta-analysis.
Loading..
Loading..
Figure 7. Random effects meta-analysis for all studies.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Loading..
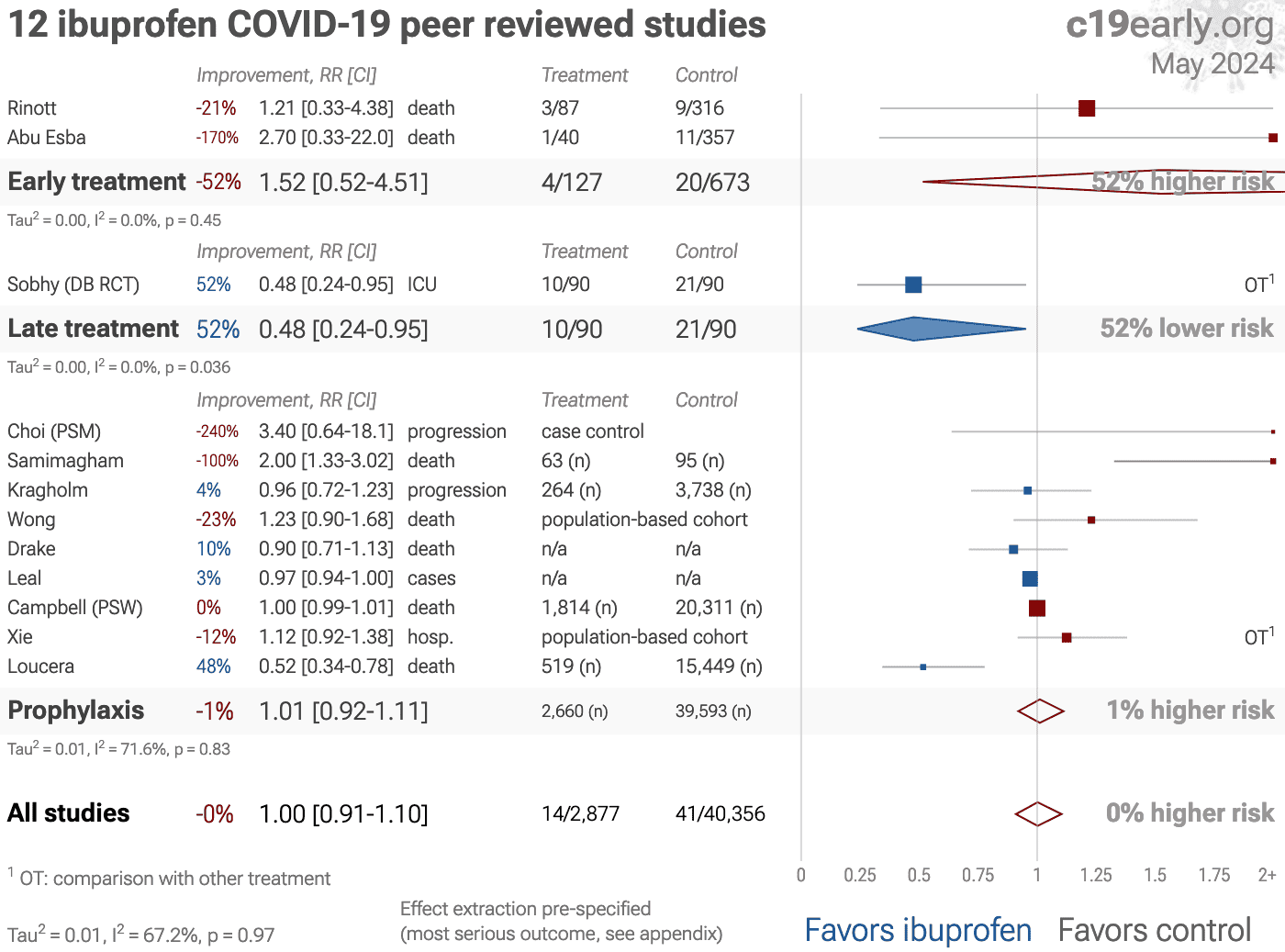
Figure 15. Random effects meta-analysis for peer reviewed studies.
Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Zeraatkar et al. analyze 356 COVID-19 trials, finding no significant
evidence that preprint results are inconsistent with peer-reviewed studies.
They also show extremely long peer-review delays, with a median of 6 months to
journal publication. A six month delay was equivalent to around 1.5 million
deaths during the first two years of the pandemic. Authors recommend using
preprint evidence, with appropriate checks for potential falsified data, which
provides higher certainty much earlier. Davidson et al. also showed no
important difference between meta analysis results of preprints and
peer-reviewed publications for COVID-19, based on 37 meta analyses including
114 trials.
{kind=link}
Loading..
Figure 16. Random effects meta-analysis for non-symptomatic vs. symptomatic results.
Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below.
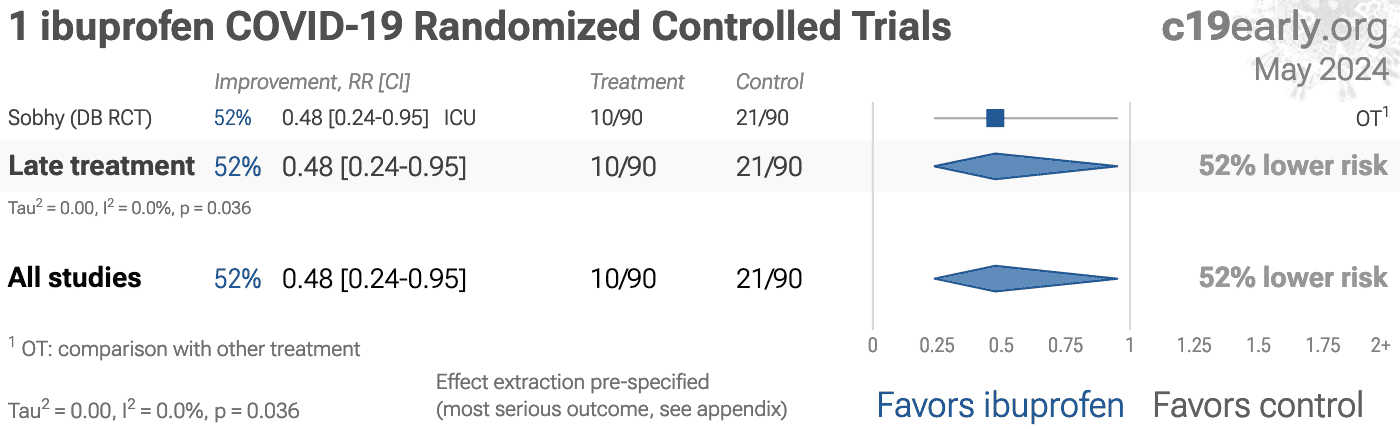
Figure 17 shows a forest plot for random
effects meta-analysis of all Randomized Controlled Trials.
RCT results are included in Table 1 and Table 2.
Currently there is only one RCT.
RCTs help to make study groups more similar and can provide a higher level of
evidence, however they are subject to many biases46, and
analysis of double-blind RCTs has identified extreme levels of bias47.
For COVID-19, the overhead may delay treatment, dramatically compromising
efficacy; they may encourage monotherapy for simplicity at the cost of
efficacy which may rely on combined or synergistic effects; the participants
that sign up may not reflect real world usage or the population that benefits
most in terms of age, comorbidities, severity of illness, or other factors;
standard of care may be compromised and unable to evolve quickly based on
emerging research for new diseases; errors may be made in randomization and
medication delivery; and investigators may have hidden agendas or vested
interests influencing design, operation, analysis, reporting, and the
potential for fraud. All of these biases have been observed with COVID-19
RCTs. There is no guarantee that a specific RCT provides a higher level of
evidence.
RCTs are expensive and many RCTs are funded
by pharmaceutical companies or interests closely aligned with pharmaceutical
companies. For COVID-19, this creates an incentive to show efficacy for
patented commercial products, and an incentive to show a lack of efficacy for
inexpensive treatments. The bias is expected to be significant, for example
Als-Nielsen et al. analyzed 370 RCTs from Cochrane reviews, showing that
trials funded by for-profit organizations were 5 times more likely to
recommend the experimental drug compared with those funded by nonprofit
organizations. For COVID-19, some major philanthropic organizations are
largely funded by investments with extreme conflicts of interest for and
against specific COVID-19 interventions.
High quality RCTs for novel acute diseases are more challenging, with
increased ethical issues due to the urgency of treatment, increased risk due
to enrollment delays, and more difficult design with a rapidly evolving
evidence base. For COVID-19, the most common site of initial infection is the
upper respiratory tract. Immediate treatment is likely to be most successful
and may prevent or slow progression to other parts of the body. For a
non-prophylaxis RCT, it makes sense to provide treatment in advance and
instruct patients to use it immediately on symptoms, just as some governments
have done by providing medication kits in advance. Unfortunately, no RCTs have
been done in this way. Every treatment RCT to date involves delayed treatment.
Among the 172 treatments we have analyzed,
67% of RCTs involve very late treatment 5+ days after
onset. No non-prophylaxis COVID-19 RCTs match the potential real-world use of
early treatments. They may more accurately represent results for treatments
that require visiting a medical facility, e.g., those requiring intravenous
administration.
{kind=link}
Figure 18.
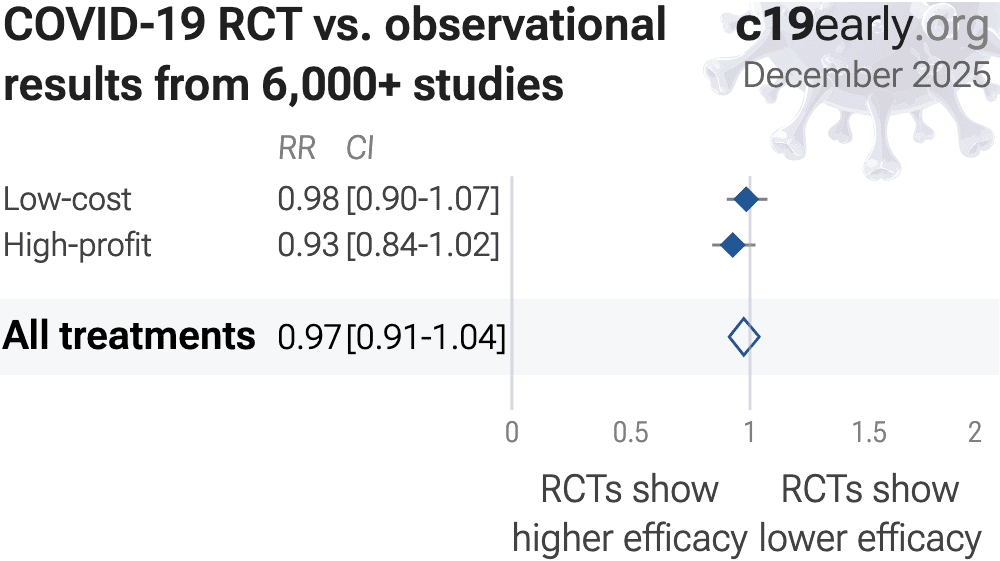
For COVID-19, observational study results do not systematically
differ from RCTs, RR 0.98 [0.92‑1.05]
across 172 treatments49.
Evidence shows that observational studies
can also provide reliable results. Concato et al. found that well-designed
observational studies do not systematically overestimate the magnitude of the
effects of treatment compared to RCTs. Anglemyer et al. analyzed reviews
comparing RCTs to observational studies and found little evidence for
significant differences in effect estimates.
We performed a similar analysis across the 172 treatments
we cover, showing no significant difference in the results of RCTs compared to
observational studies, RR 0.98 [0.92‑1.05]52. Similar results are found for all low-cost treatments, RR
1.00 [0.91‑1.09]. High-cost treatments
show a non-significant trend towards RCTs showing greater efficacy,
RR 0.92 [0.84‑1.02].
Details can be found in the
supplementary data.
Lee et al. showed that only 14% of the guidelines of the Infectious
Diseases Society of America were based on RCTs. Evaluation of studies relies
on an understanding of the study and potential biases. Limitations in an RCT
can outweigh the benefits, for example excessive dosages, excessive treatment
delays, or remote survey bias may have a greater effect on results. Ethical
issues may also prevent running RCTs for known effective treatments. For more
on issues with RCTs see54,55.
Currently, 55 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. Of these, 58% have been confirmed in RCTs, with a mean delay of 7.7 months (64% with 8.9 months delay for low-cost treatments). The remaining treatments either have no RCTs, or the point estimate is consistent.
We need to evaluate each trial on its own merits. RCTs for a
given medication and disease may be more reliable, however they may also be
less reliable. For off-patent medications, very high conflict of interest
trials may be more likely to be RCTs, and more likely to be large trials that
dominate meta analyses.
{kind=link}
Loading..
Figure 17. Random effects meta-analysis for all Randomized Controlled Trials.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
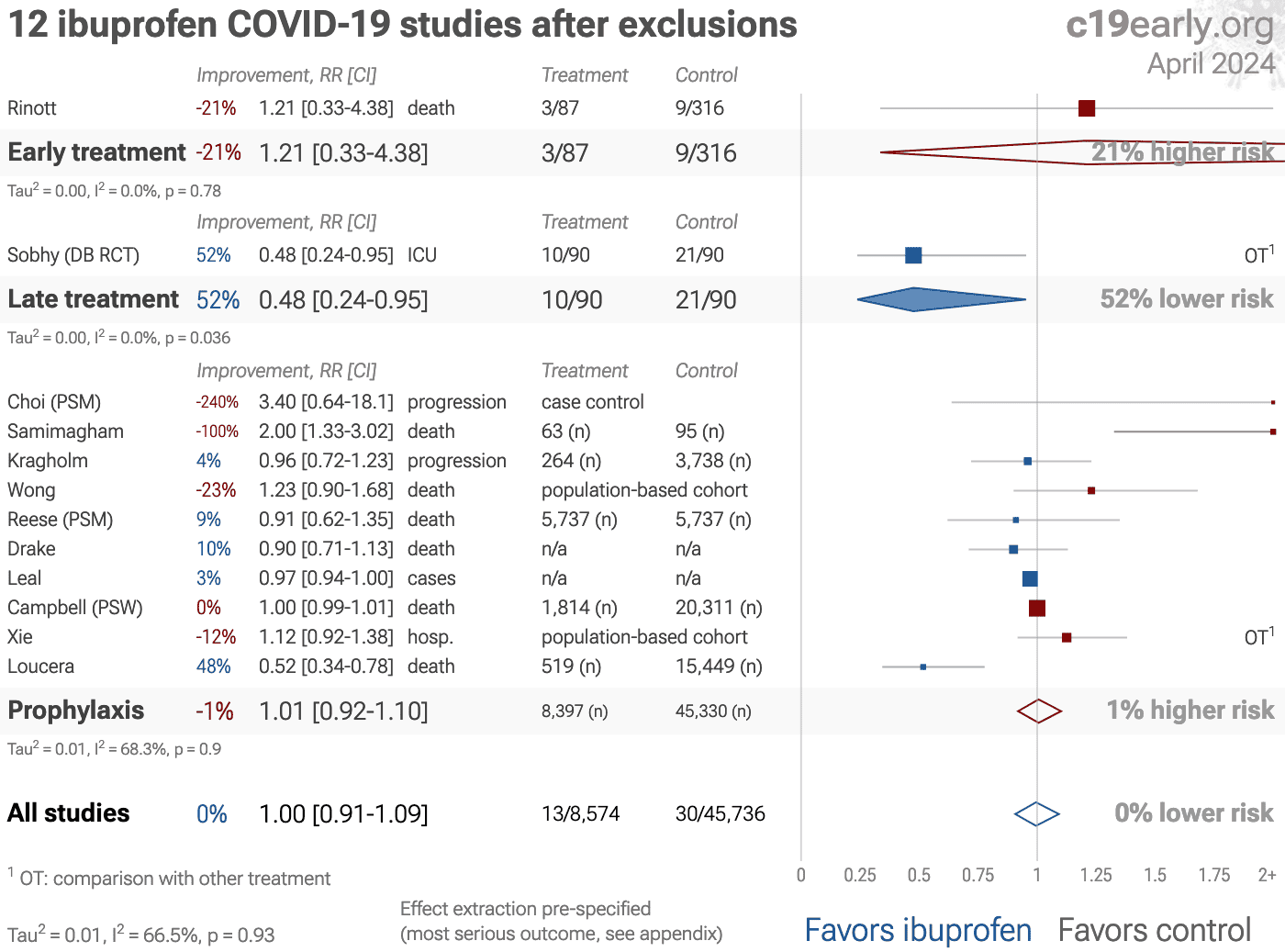
To avoid bias in the selection of studies, we analyze all
non-retracted studies. Here we show the results after excluding
studies with major issues likely to alter results, non-standard studies, and
studies where very minimal detail is currently available. Our bias evaluation
is based on analysis of each study and identifying when there is a significant
chance that limitations will substantially change the outcome of the study. We
believe this can be more valuable than checklist-based approaches such as
Cochrane GRADE, which can be easily influenced by potential bias, may ignore
or underemphasize serious issues not captured in the checklists, and may
overemphasize issues unlikely to alter outcomes in specific cases (for example
certain specifics of randomization with a very large effect size and
well-matched baseline characteristics).
The studies excluded are as below.
Figure 19 shows a forest plot for random
effects meta-analysis of all studies after exclusions.
Abu Esba, substantial unadjusted confounding by indication likely.
{kind=link}
Loading..
Figure 19. Random effects meta-analysis for all studies after exclusions.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
Heterogeneity in COVID-19 studies arises from many factors including:
The time between infection or the onset of symptoms and
treatment may critically affect how well a treatment works. For example an
antiviral may be very effective when used early but may not be effective in
late stage disease, and may even be harmful. Oseltamivir, for example, is
generally only considered effective for influenza when used within 0-36 or
0-48 hours57,58. Baloxavir marboxil studies for influenza
also show that treatment delay is critical — Ikematsu et al. report
an 86% reduction in cases for post-exposure prophylaxis, Hayden et al.
show a 33 hour reduction in the time to alleviation of symptoms for treatment
within 24 hours and a reduction of 13 hours for treatment within 24-48 hours,
and Kumar et al. report only 2.5 hours improvement for inpatient
treatment.
| Treatment delay | Result |
| Post-exposure prophylaxis | 86% fewer cases59 |
| <24 hours | -33 hours symptoms60 |
| 24-48 hours | -13 hours symptoms60 |
| Inpatients | -2.5 hours to improvement61 |
Figure 20 shows a mixed-effects meta-regression for efficacy
as a function of treatment delay in COVID-19 studies from 172 treatments, showing
that efficacy declines rapidly with treatment delay. Early treatment is
critical for COVID-19.
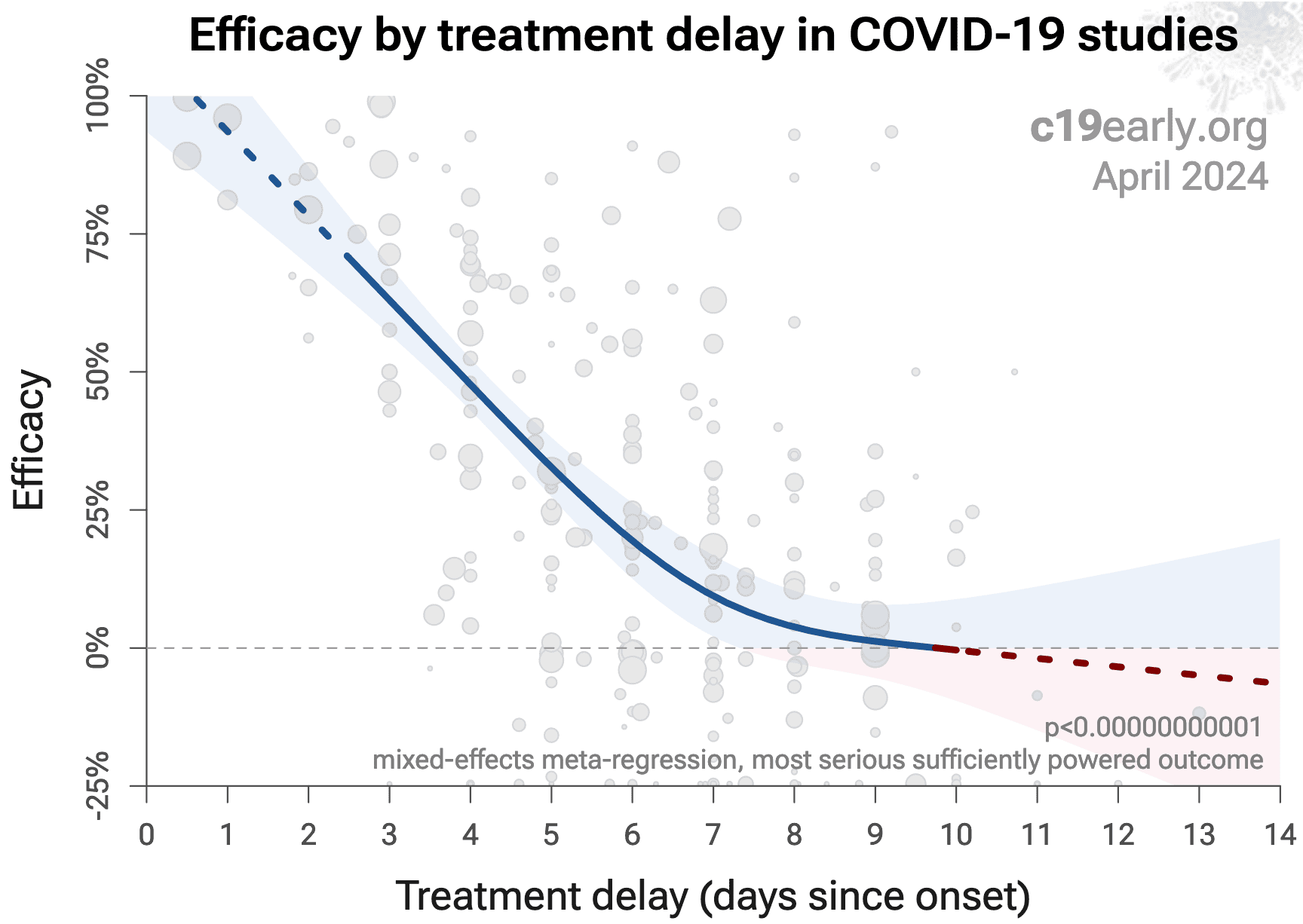{kind=link}
Figure 20. Early treatment is more effective. Meta-regression showing efficacy as a function of treatment delay in COVID-19 studies from 172 treatments.
Details of the patient population including age and comorbidities may
critically affect how well a treatment works. For example, many COVID-19
studies with relatively young low-comorbidity patients show all patients
recovering quickly with or without treatment. In such cases, there is little
room for an effective treatment to improve results, for example as in
López-Medina et al.
Efficacy may depend critically on the distribution of
SARS-CoV-2 variants encountered by patients. Risk varies significantly across
variants63, for example the Gamma variant shows significantly
different characteristics64-67. Different
mechanisms of action may be more or less effective depending on variants, for
example the degree to which TMPRSS2 contributes to viral entry can differ
across variants68,69.
Effectiveness may depend strongly on the dosage and treatment regimen.
The quality of medications may vary significantly between
manufacturers and production batches, which may significantly affect efficacy
and safety. Williams et al. analyze ivermectin from 11 different sources,
showing highly variable antiparasitic efficacy across different manufacturers.
Xu et al. analyze a treatment from two different manufacturers, showing 9
different impurities, with significantly different concentrations for each
manufacturer.
Across all
studies there is a strong association between different outcomes, for example
improved recovery is strongly associated with lower mortality. However,
efficacy may differ depending on the effect measured, for example a treatment
may be more effective against secondary complications and have minimal effect
on viral clearance.
The
distribution of studies will alter the outcome of a meta analysis. Consider a
simplified example where everything is equal except for the treatment delay,
and effectiveness decreases to zero or below with increasing delay. If there
are many studies using very late treatment, the outcome may be negative, even
though early treatment is very effective.
All meta analyses combine heterogeneous studies, varying in population,
variants, and potentially all factors above, and therefore may obscure
efficacy by including studies where treatment is less effective. Generally, we
expect the estimated effect size from meta analysis to be less than that for
the optimal case.
Looking at all studies is valuable for providing an overview of all research,
important to avoid cherry-picking, and informative when a positive result is
found despite combining less-optimal situations. However, the resulting
estimate does not apply to specific cases such as
early treatment in high-risk populations.
While we present results for all studies, we also present treatment time and
individual outcome analyses, which may be more informative for specific use
cases.
For COVID-19, delay in clinical results translates into
additional death and morbidity, as well as additional economic and societal
damage. Combining the results of studies reporting different outcomes is
required.
There may be no mortality in a trial with low-risk patients,
however a reduction in severity or improved viral clearance may translate
into lower mortality in a high-risk population.
Different studies may report lower severity, improved recovery, and lower mortality,
and the significance may be very high when combining the results.
"The studies reported different outcomes" is not a good reason for
disregarding results.
Pooling the results of studies reporting different outcomes allows us to use
more of the available information. Logically we should, and do, use additional
information when evaluating treatments—for example dose-response and
treatment delay-response relationships provide additional evidence of efficacy
that is considered when reviewing the evidence for a treatment.
We present both specific outcome and pooled analyses.
In order to combine the results of studies reporting different outcomes we use
the most serious outcome reported in each study, based on the thesis that
improvement in the most serious outcome provides comparable measures of
efficacy for a treatment. A critical advantage of this approach is
simplicity and transparency.
There are many other ways to combine evidence for different outcomes, along
with additional evidence such as dose-response relationships, however these
increase complexity.
Trials with high-risk patients may be restricted due to ethics for treatments
that are known or expected to be effective, and they increase difficulty for
recruiting. Using less severe outcomes as a proxy for more serious outcomes
allows faster and safer collection of evidence.
For many COVID-19 treatments, a reduction in mortality logically
follows from a reduction in hospitalization, which follows from a reduction in
symptomatic cases, which follows from a reduction in PCR positivity. We can
directly test this for COVID-19.
Analysis of the the association between different outcomes across studies from
all 172
treatments we cover confirms the validity of pooled outcome analysis for COVID-19.
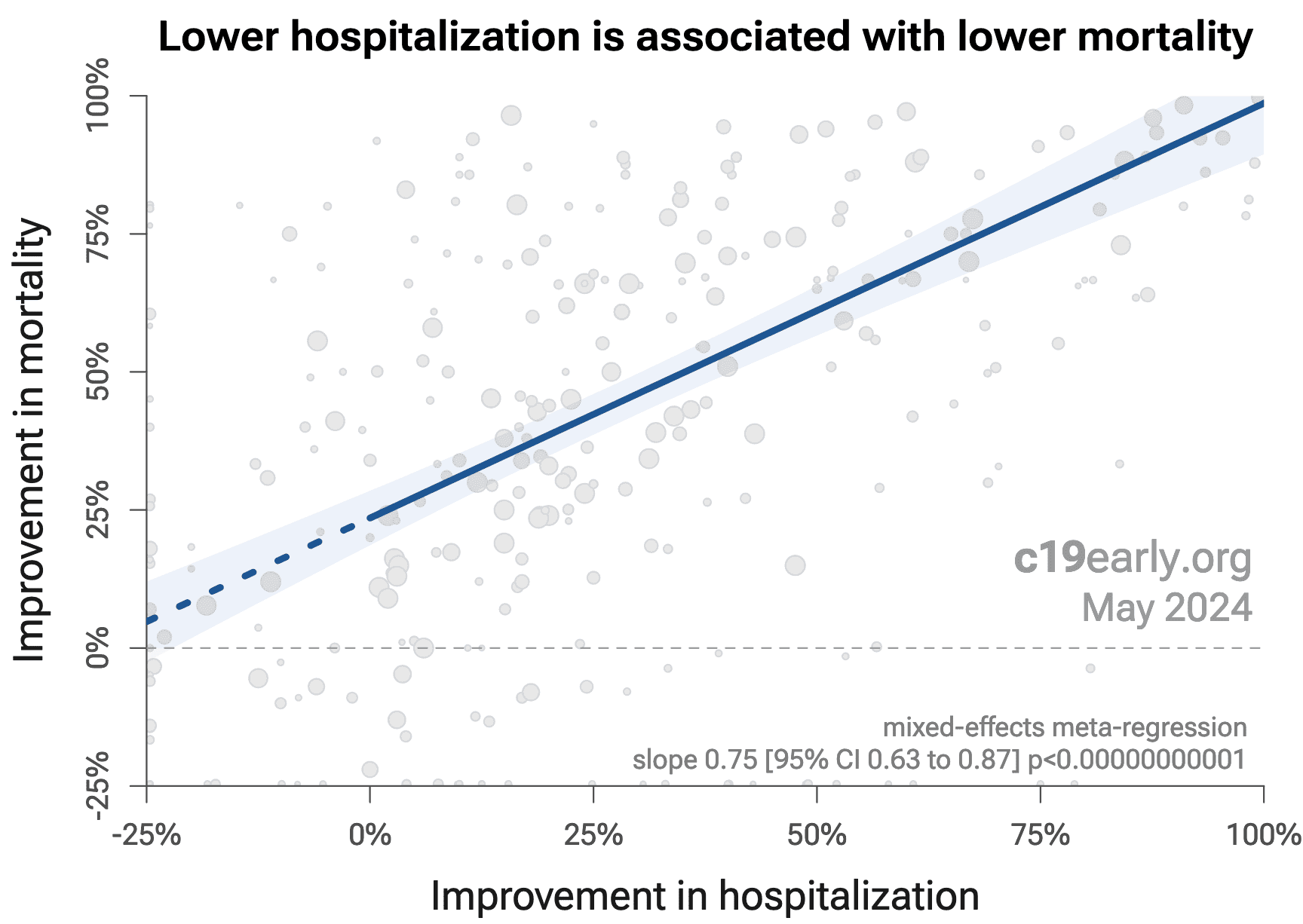
Figure 21 shows that lower hospitalization is very strongly associated
with lower mortality (p < 0.000000000001).
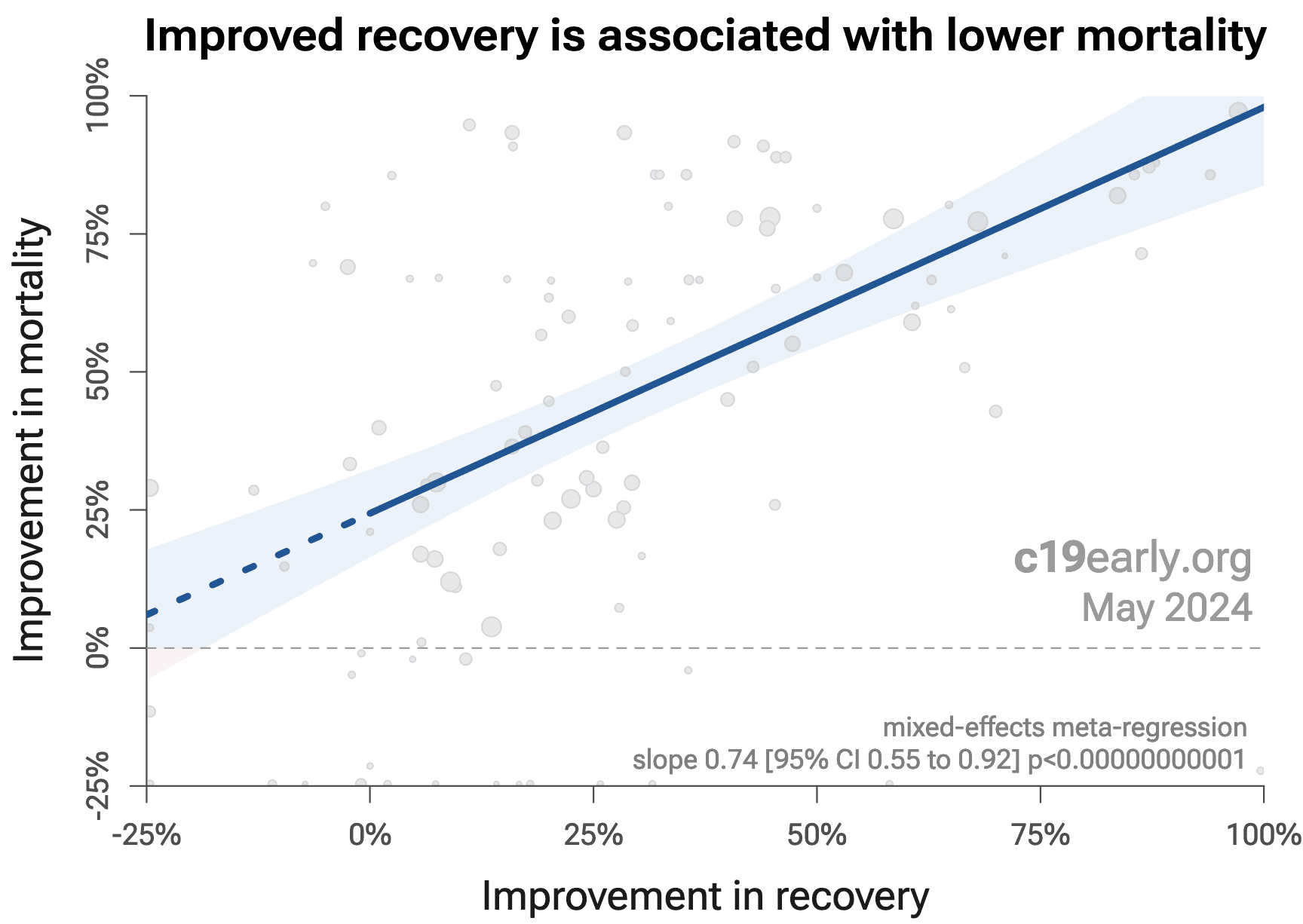
Similarly, Figure 22 shows that improved recovery is very strongly associated
with lower mortality (p < 0.000000000001).
Considering the extremes, Singh et al. show an association between viral clearance and
hospitalization or death, with p = 0.003 after excluding one large
outlier from a mutagenic treatment, and based on 44 RCTs including 52,384
patients.
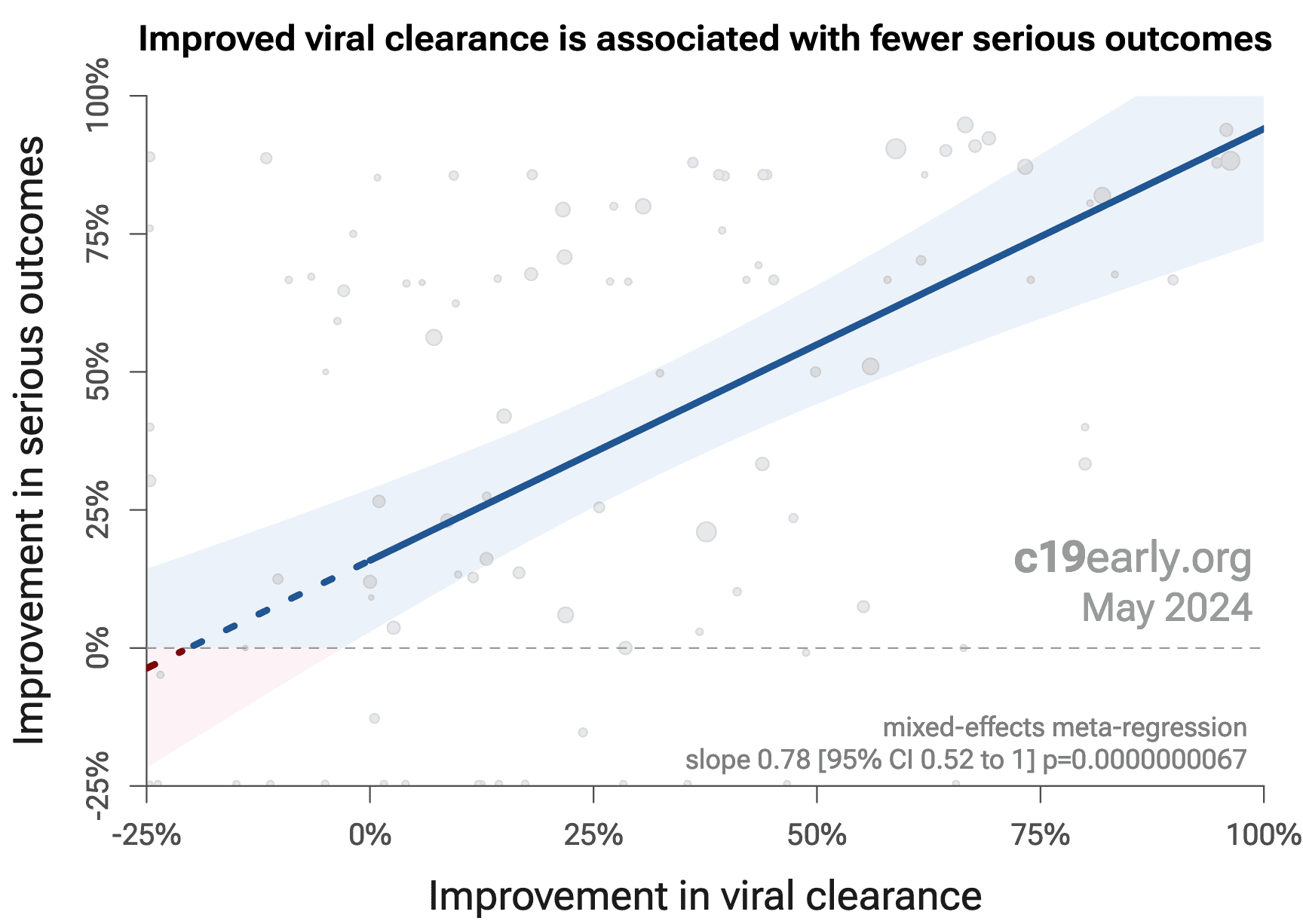
Figure 23 shows that improved viral clearance is strongly associated
with fewer serious outcomes. The association is very similar to
Singh et al., with higher confidence due to the larger number of
studies. As with Singh et al., the confidence increases
when excluding the outlier treatment, from p = 0.000000082 to p = 0.0000000033.
{kind=link}
Figure 21. Lower hospitalization is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Figure 22. Improved recovery is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Figure 21. Improved viral clearance is associated with fewer serious outcomes, supporting pooled outcome analysis.
Currently, 55 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. 88% of these have been confirmed with one or more specific outcomes, with a mean delay of 4.9 months. When restricting to RCTs only, 57% of treatments showing statistically significant efficacy/harm with pooled effects have been confirmed with one or more specific outcomes, with a mean delay of 7.3 months.
Figure 24 shows when treatments were found effective during the
pandemic. Pooled outcomes often resulted in earlier detection of efficacy.
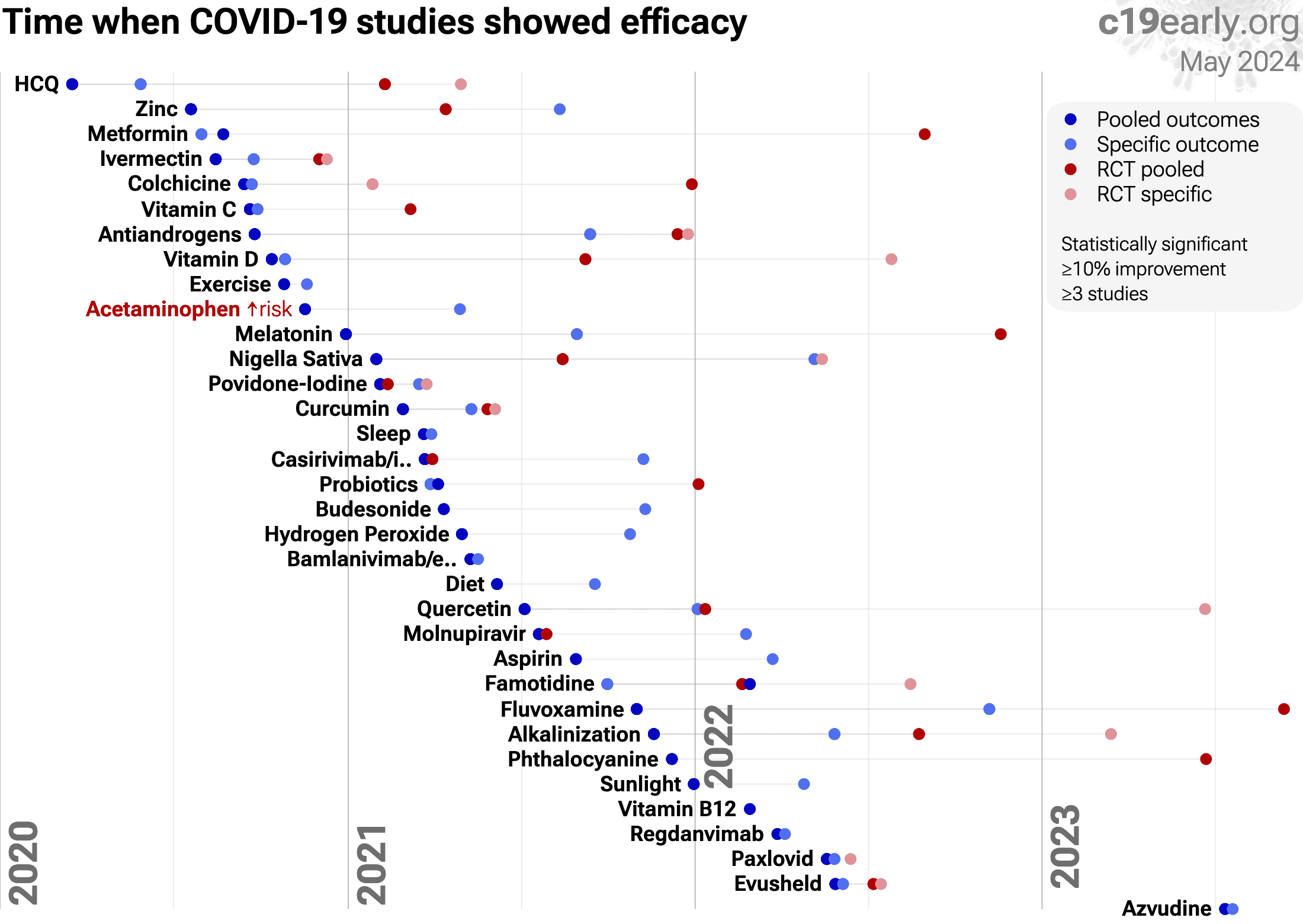{kind=link}
Figure 24. The time when studies showed that
treatments were effective, defined as statistically significant improvement of
≥10% from ≥3 studies.
Pooled results typically show efficacy earlier than specific
outcome results. Results from all studies often shows efficacy much earlier
than when restricting to RCTs.
Results reflect conditions as used in trials to date, these depend on the
population treated, treatment delay, and treatment regimen.
Pooled analysis could hide efficacy, for example a treatment that is
beneficial for late stage patients but has no effect on viral clearance may
show no efficacy if most studies only examine viral clearance. In practice, it
is rare for a non-antiviral treatment to report viral clearance and to not
report clinical outcomes; and in practice other sources of heterogeneity such
as difference in treatment delay is more likely to hide efficacy.
Analysis validates the use of pooled effects and shows significantly faster
detection of efficacy on average.
However, as with all meta analyses, it is important to review the different
studies included. We also present individual outcome analyses, which may be
more informative for specific use cases.
Publishing is often biased
towards positive results, however evidence suggests that there may be a negative bias for
inexpensive treatments for COVID-19. Both negative and positive results are
very important for COVID-19, media in many countries prioritizes negative
results for inexpensive treatments (inverting the typical incentive for
scientists that value media recognition), and there are many reports of
difficulty publishing positive results90-93.
For ibuprofen, there is currently not
enough data to evaluate publication bias with high confidence.
Funnel
plots have traditionally been used for analyzing publication bias. This is
invalid for COVID-19 acute treatment trials — the underlying assumptions
are invalid, which we can demonstrate with a simple example. Consider a set of
hypothetical perfect trials with no bias. Figure 25 plot A
shows a funnel plot for a simulation of 80 perfect trials, with random group
sizes, and each patient's outcome randomly sampled (10% control event
probability, and a 30% effect size for treatment). Analysis shows no asymmetry
(p > 0.05). In plot B, we add a single typical variation in COVID-19 treatment
trials — treatment delay. Consider that efficacy varies from 90% for
treatment within 24 hours, reducing to 10% when treatment is delayed 3 days.
In plot B, each trial's treatment delay is randomly selected. Analysis now
shows highly significant asymmetry, p < 0.0001, with six variants of
Egger's test all showing p < 0.0594-101.
Note that these tests fail even though treatment delay is uniformly
distributed. In reality treatment delay is more complex — each trial has
a different distribution of delays across patients, and the distribution
across trials may be biased (e.g., late treatment trials may be more common).
Similarly, many other variations in trials may produce asymmetry, including
dose, administration, duration of treatment, differences in SOC,
comorbidities, age, variants, and bias in design, implementation, analysis,
and reporting.
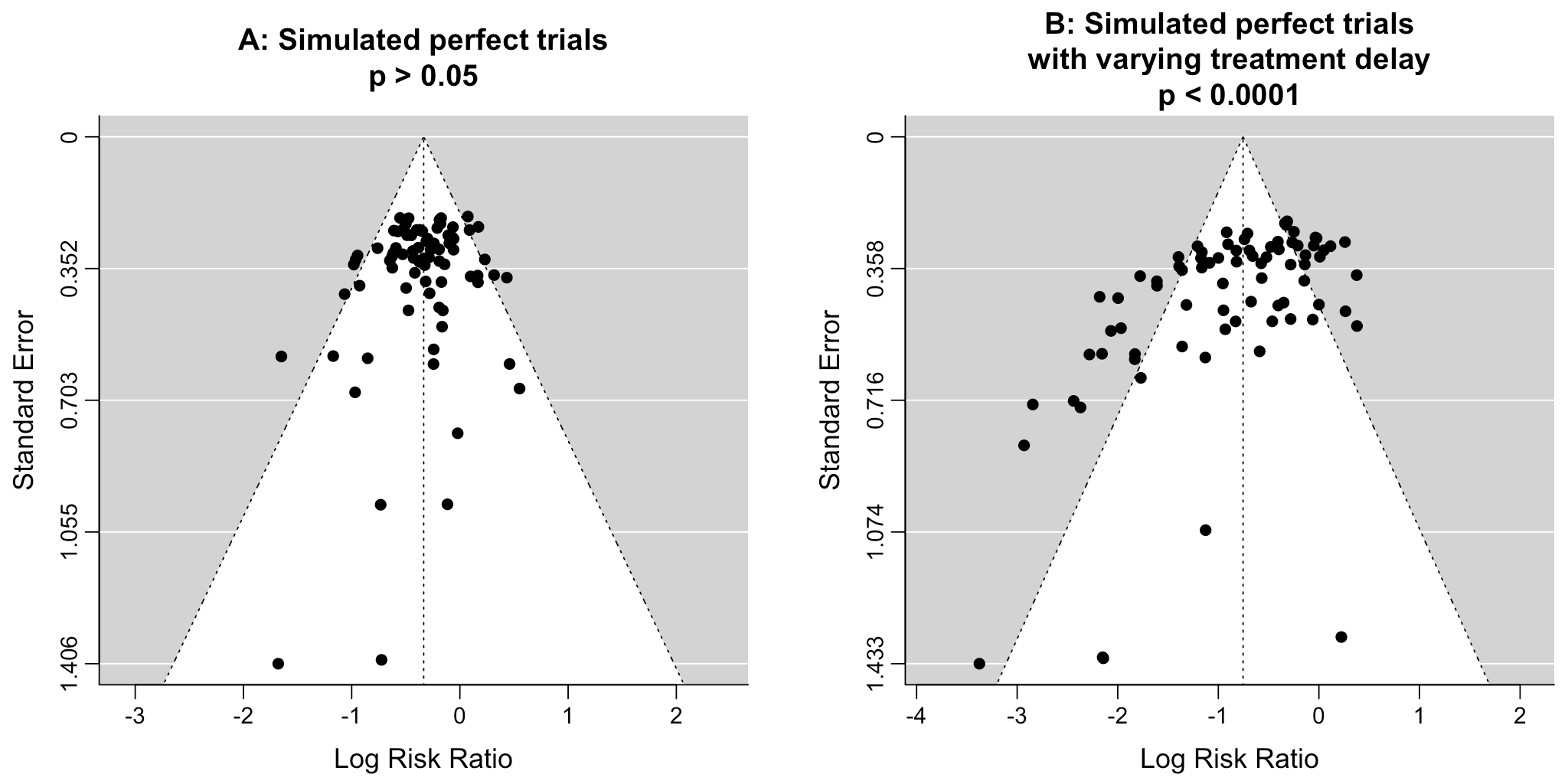{kind=link}
Figure 25. Example funnel plot analysis for simulated perfect trials.
Pharmaceutical drug
trials often have conflicts of interest whereby sponsors or trial staff have a
financial interest in the outcome being positive. Ibuprofen for COVID-19
lacks this because it is off-patent, has multiple manufacturers, and is very low cost.
In contrast, most COVID-19 ibuprofen trials have been run by
physicians on the front lines with the primary goal of finding the best
methods to save human lives and minimize the collateral damage caused by
COVID-19. While pharmaceutical companies are careful to run trials under
optimal conditions (for example, restricting patients to those most likely to
benefit, only including patients that can be treated soon after onset when
necessary, and ensuring accurate dosing), not all ibuprofen trials
represent the optimal conditions for efficacy.
Summary statistics from
meta analysis necessarily lose information. As with all meta analyses, studies
are heterogeneous, with differences
in treatment delay, treatment regimen, patient demographics, variants,
conflicts of interest, standard of care, and other factors. We provide analyses for specific
outcomes and by treatment delay, and we aim to identify key characteristics in
the forest plots and summaries. Results should be viewed in the context of
study characteristics.
Some analyses classify treatment based on early or late
administration, as done here, while others distinguish between mild, moderate,
and severe cases. Viral load does not indicate degree of symptoms — for
example patients may have a high viral load while being asymptomatic. With
regard to treatments that have antiviral properties, timing of treatment is
critical — late administration may be less helpful regardless of
severity.
Details of treatment delay per patient is often not available.
For example, a study may treat 90% of patients relatively early, but the
events driving the outcome may come from 10% of patients treated very late.
Our 5 day cutoff for early treatment may be too conservative, 5 days may be too late in many cases.
Comparison across treatments is confounded by differences in
the studies performed, for example dose, variants, and conflicts of interest.
Trials with conflicts of interest may use designs better suited to the
preferred outcome.
In some cases, the most serious outcome has very few events,
resulting in lower confidence results being used in pooled analysis, however
the method is simpler and more transparent. This is less critical as the
number of studies increases. Restriction to outcomes with sufficient power may
be beneficial in pooled analysis and improve accuracy when there are few
studies, however we maintain our pre-specified method to avoid any
retrospective changes.
Studies show that combinations of treatments can be highly
synergistic and may result in many times greater efficacy than individual
treatments alone72-88.
Therefore standard of care may be critical and benefits may diminish or
disappear if standard of care does not include certain treatments.
This real-time analysis is constantly updated based on
submissions. Accuracy benefits from widespread review and submission of
updates and corrections from reviewers. Less popular treatments may receive
fewer reviews.
No treatment or intervention is 100% available and
effective for all current and future variants. Efficacy may vary significantly
with different variants and within different populations. All treatments have
potential side effects. Propensity to experience side effects may be predicted
in advance by qualified physicians. We do not provide medical advice. Before
taking any medication, consult a qualified physician who can compare all
options, provide personalized advice, and provide details of risks and
benefits based on individual medical history and situations.
2 of the 13
studies compare against other treatments, which may reduce the effect
seen.
SARS-CoV-2 infection and replication involves a complex
interplay of 100+ host and viral proteins and other
factors22-29, providing many therapeutic
targets.
Over 9,000 compounds have been predicted to reduce COVID-19
risk30, either by directly
minimizing infection or replication, by supporting immune system function, or
by minimizing secondary complications.
Figure 26 shows an overview of the results for ibuprofen
in the context of multiple COVID-19 treatments, and Figure 27 shows a plot
of efficacy vs. cost for COVID-19 treatments.
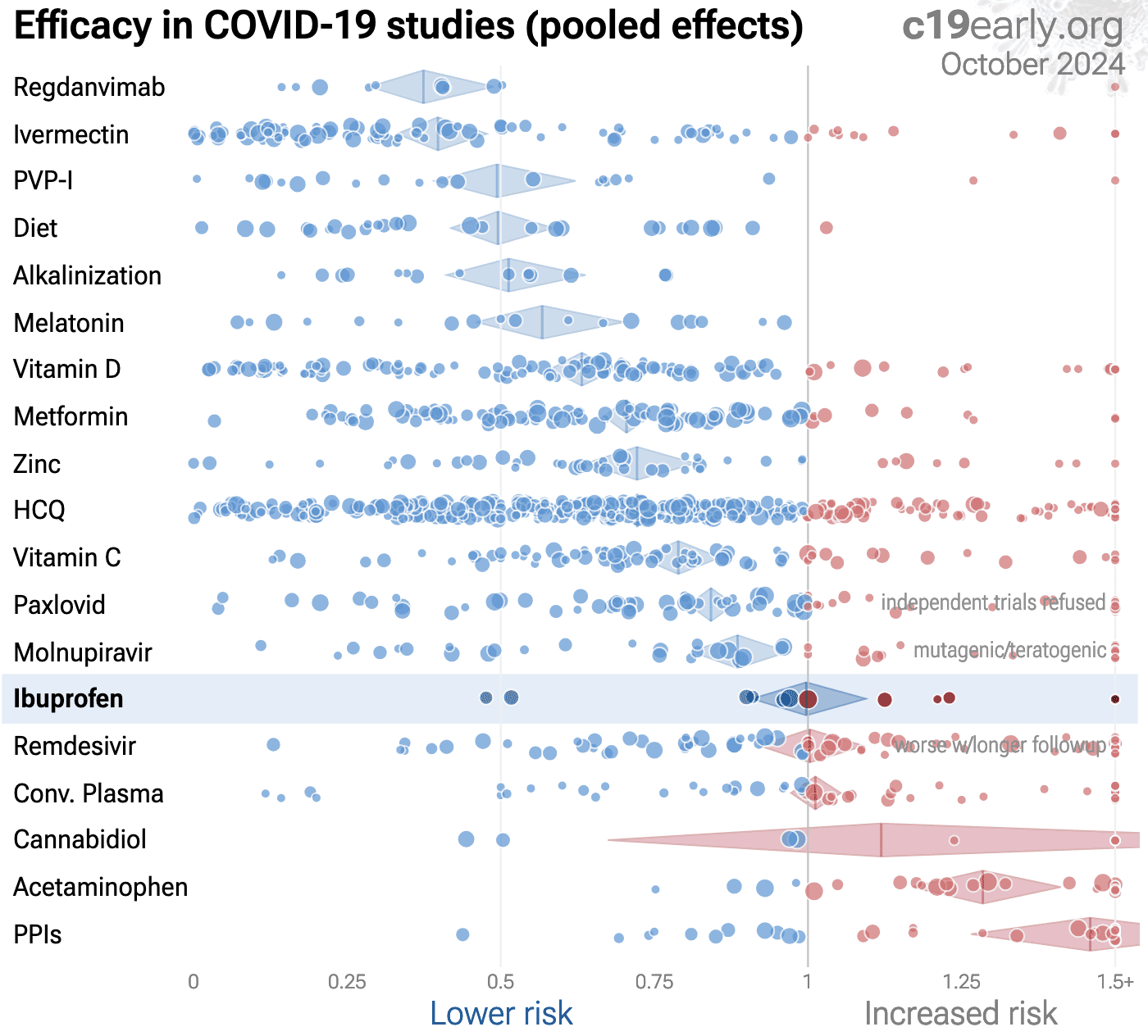{kind=link}
Figure 26.
Scatter plot showing results within the context of multiple COVID-19 treatments.
Diamonds shows the results of random effects meta-analysis.
0.6% of 9,000+ proposed treatments show efficacy133.
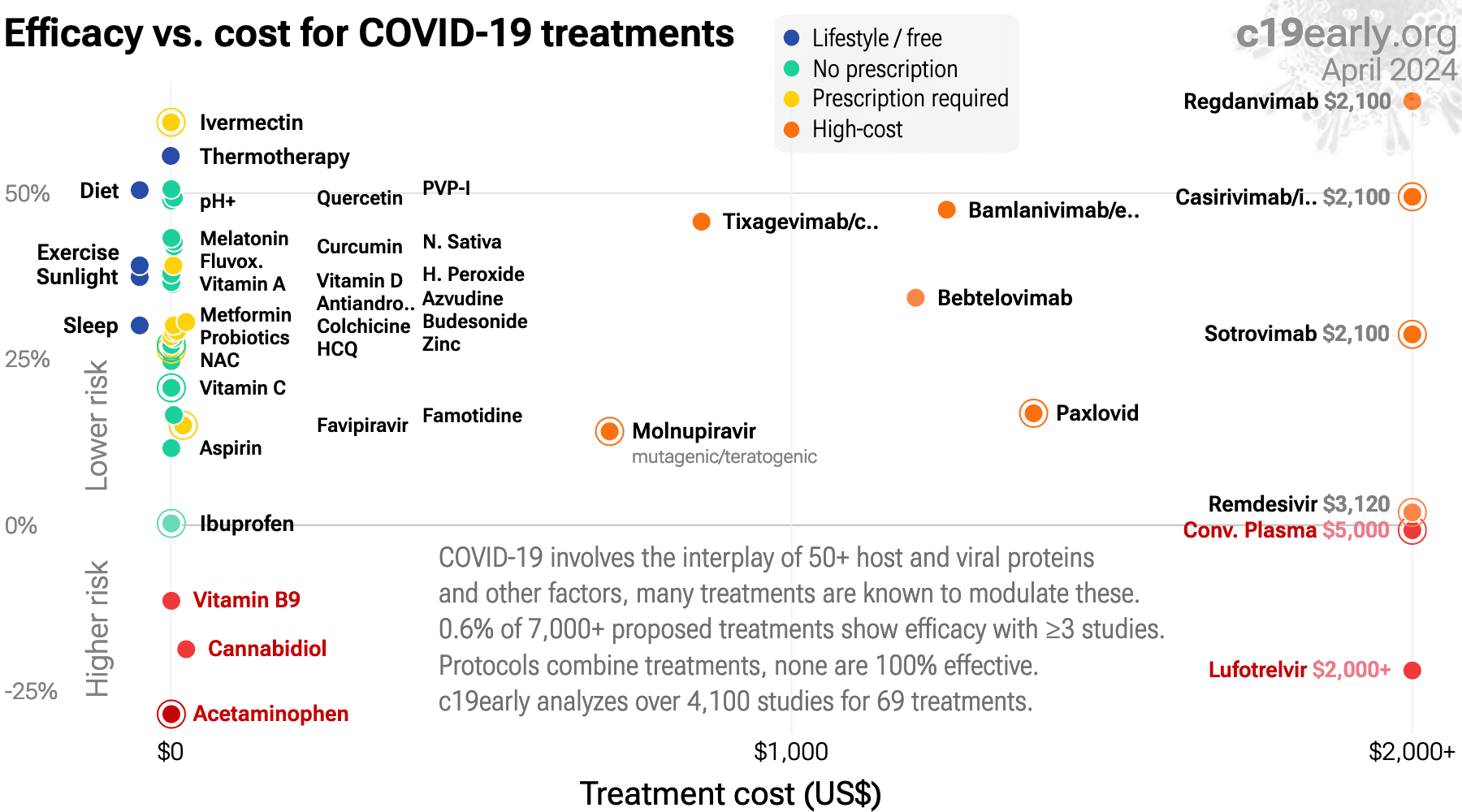{kind=link}
Figure 27. Efficacy vs. cost for COVID-19 treatments.
Meta analysis using the most serious outcome reported shows
0% [-9‑9%] lower risk, without reaching statistical significance.
4 studies from 4 independent teams in 4 countries show significant
benefit.
Concerns have been raised over potential harm with the use of ibuprofen for COVID-191 due to the suppression of beneficial immune and inflammatory responses during early infection, ACE2 upregulation, and delaying further care. There is limited clinical data currently, especially with regard to acute usage at onset of infection, however current results suggest harm with early treatment and benefit with late treatment.
{kind=link}
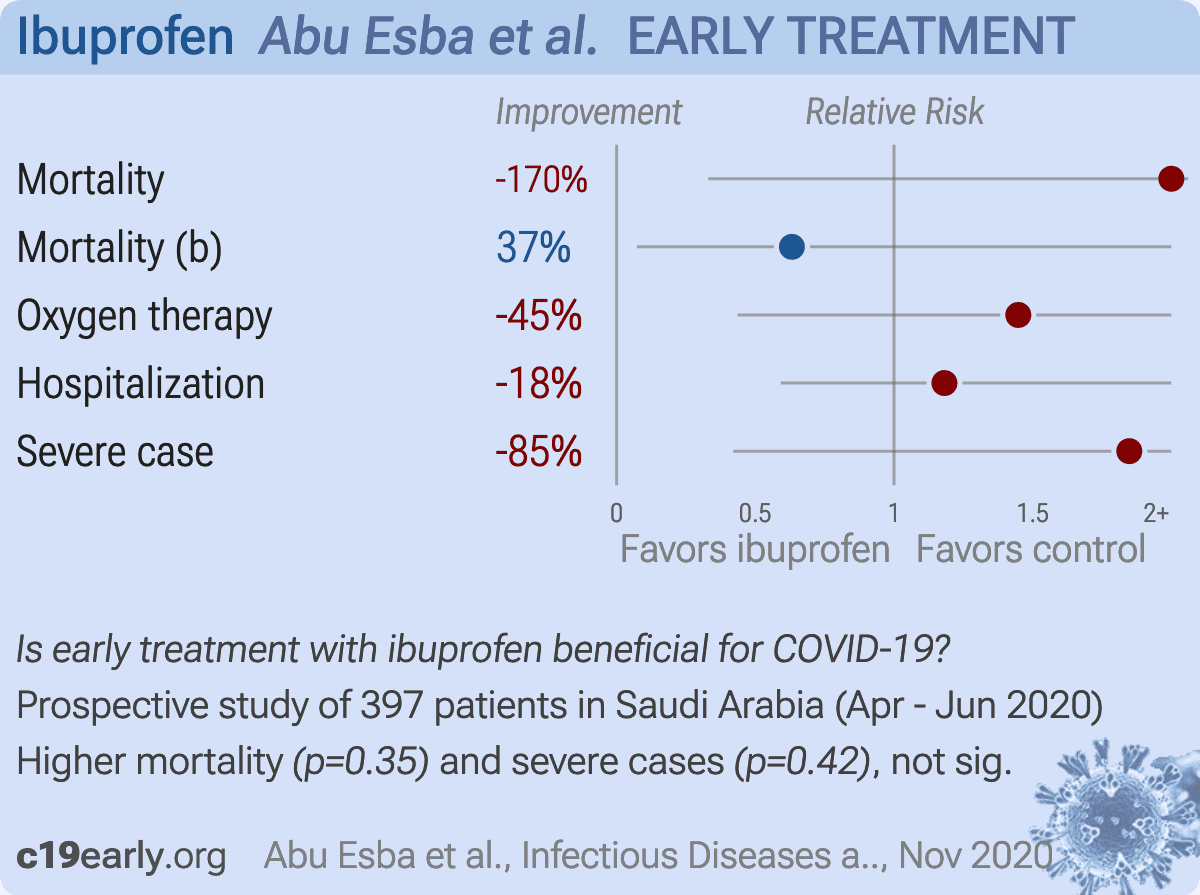
Prospective study of 503 COVID-19 cases in Saudi Arabia, 40 using ibuprofen during infection, and 357 not using NSAIDs, showing no significant differences in outcomes. Results are subject to confounding by indication.
{kind=link}
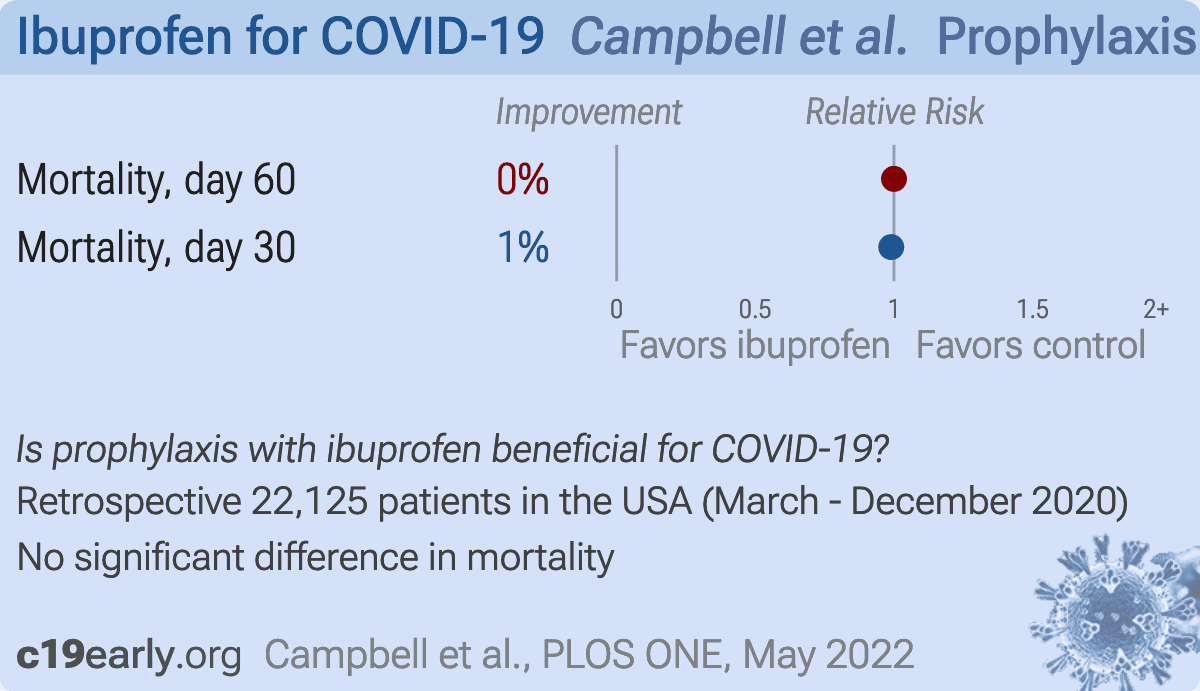
Retrospective 28,856 COVID-19 patients in the USA, showing no significant difference in mortality for chronic ibuprofen use vs. sporadic NSAID use. Since ibuprofen is available OTC and authors only tracked prescriptions, many patients classified as sporadic users may have been chronic users.
{kind=link}
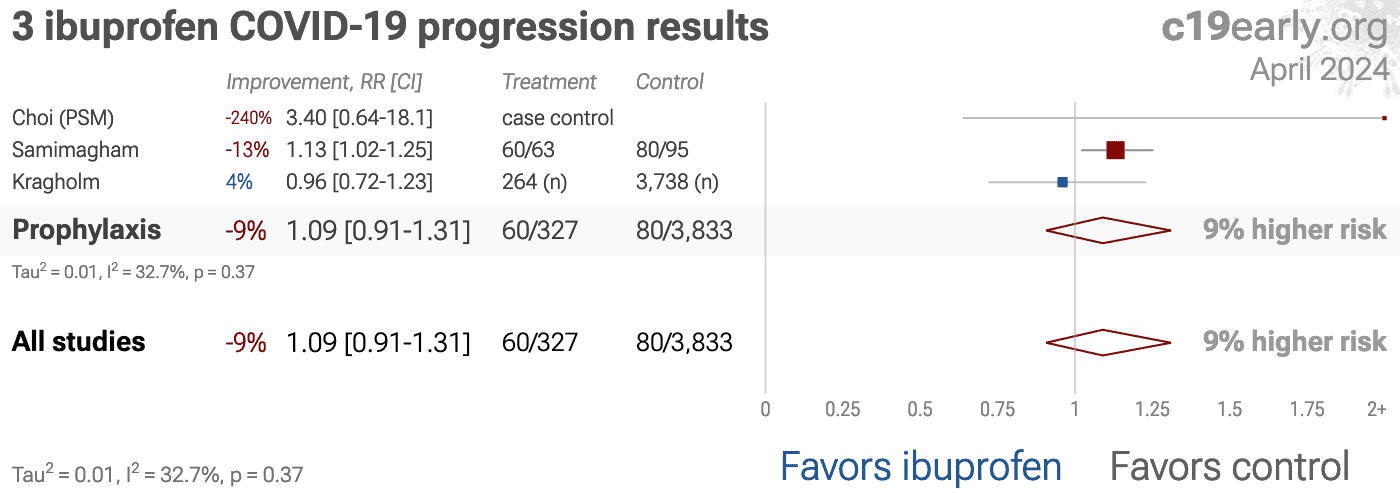
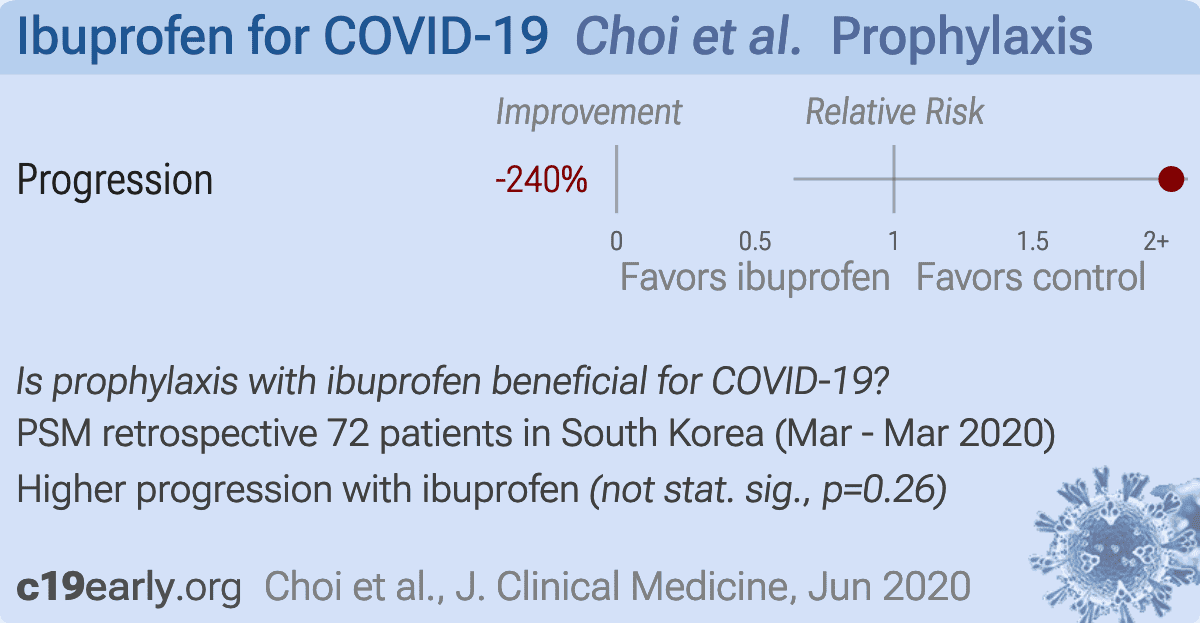
Retrospective 293 patients in South Korea, showing higher risk of progression with ibuprofen use, without statistical significance.
{kind=link}
Prospective study of 78,674 COVID-19 patients, showing no significant difference in mortality with ibuprofen use.
{kind=link}
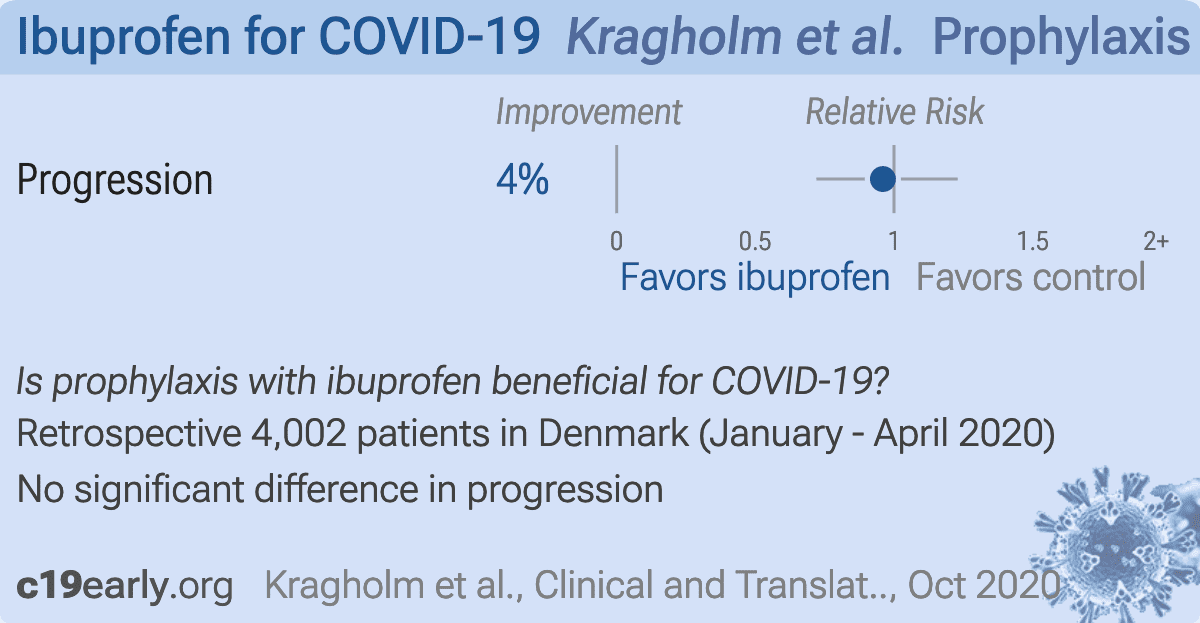
Retrospective 4,002 COVID-19 patients in Denmark, 264 with ibuprofen prescriptions, showing no significant difference for COVID-19 severity.
{kind=link}
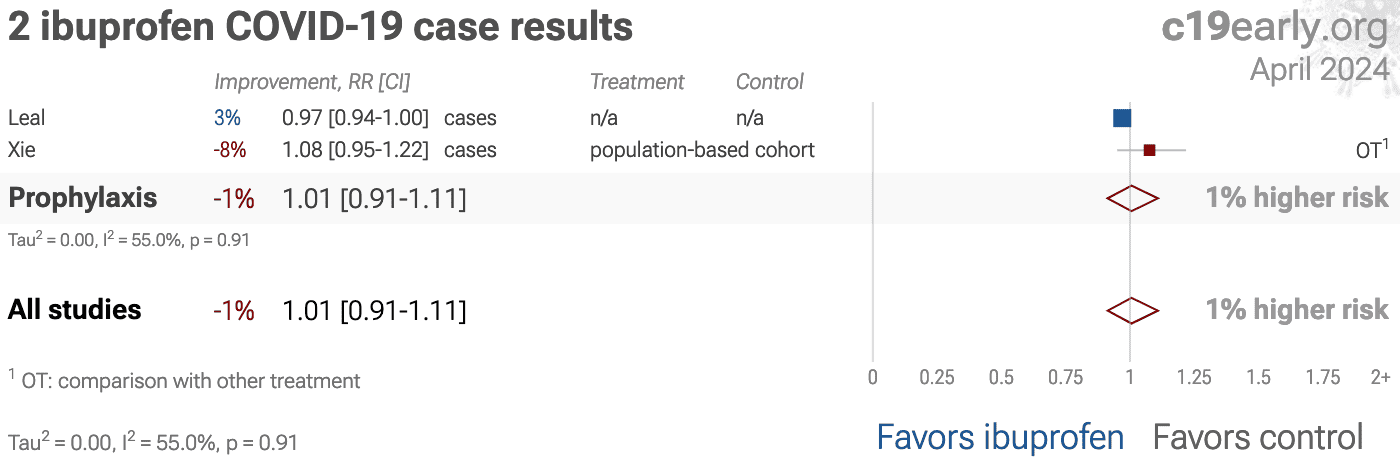
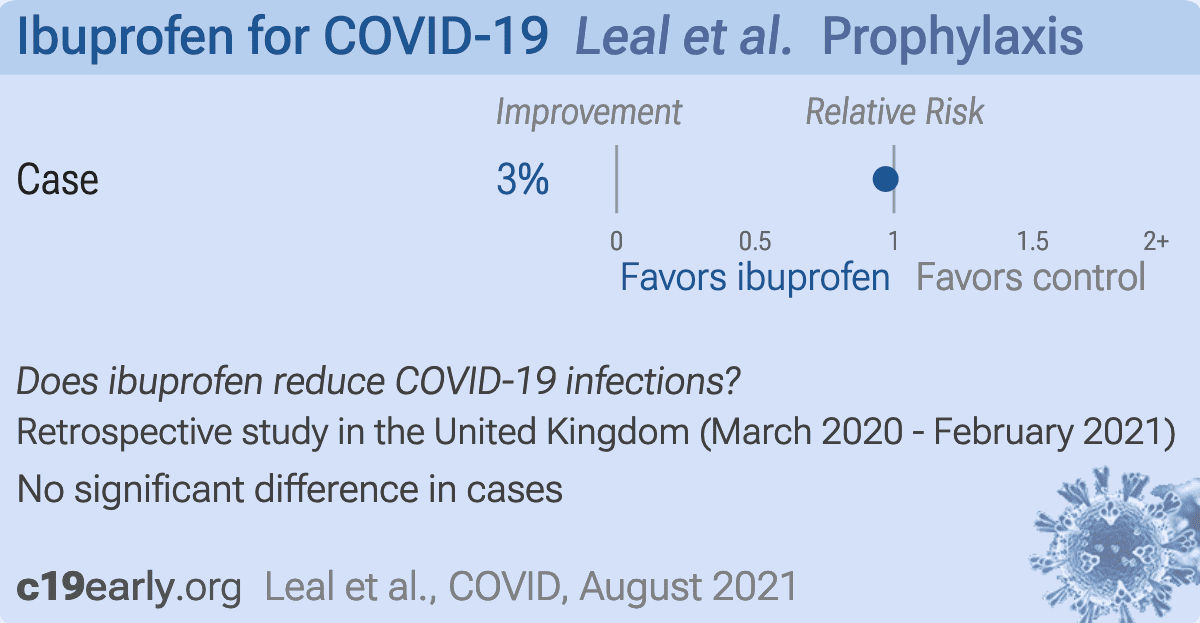
UK Biobank retrospective showing no significant difference in cases with ibuprofen use.
{kind=link}
Retrospective 15,968 COVID-19 hospitalized patients in Spain, showing lower mortality with existing use of several medications including metformin, HCQ, azithromycin, aspirin, vitamin D, vitamin C, and budesonide. Since only hospitalized patients are included, results do not reflect different probabilities of hospitalization across treatments.
{kind=link}
N3C retrospective 250,533 patients showing higher COVID-19 severity with ibuprofen use. Note that results for individual treatments are not included in the journal version or v2 of this preprint.
{kind=link}
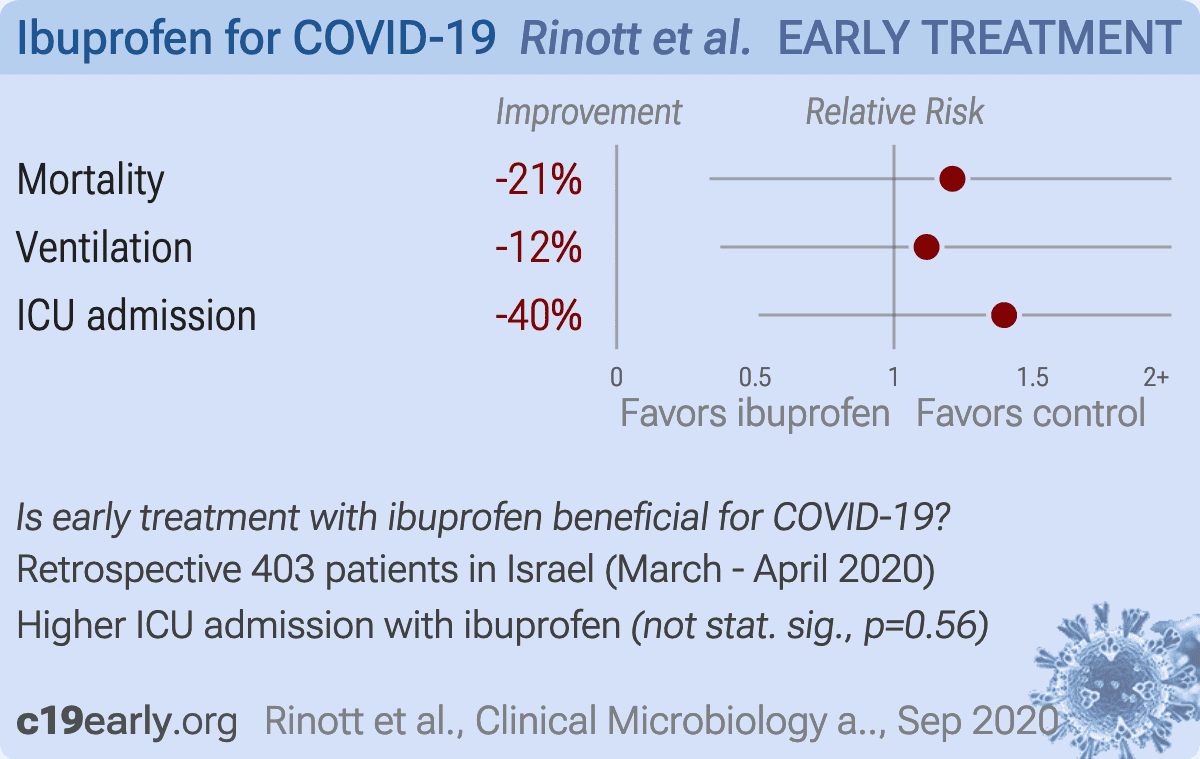
Retrospective 403 COVID-19 cases in Israel, showing no significant difference in outcomes with ibuprofen use. Patients were asked about ibuprofen use starting a week before diagnosis of COVID-19 - treatment time may have been early, late, or prophylactic.
{kind=link}
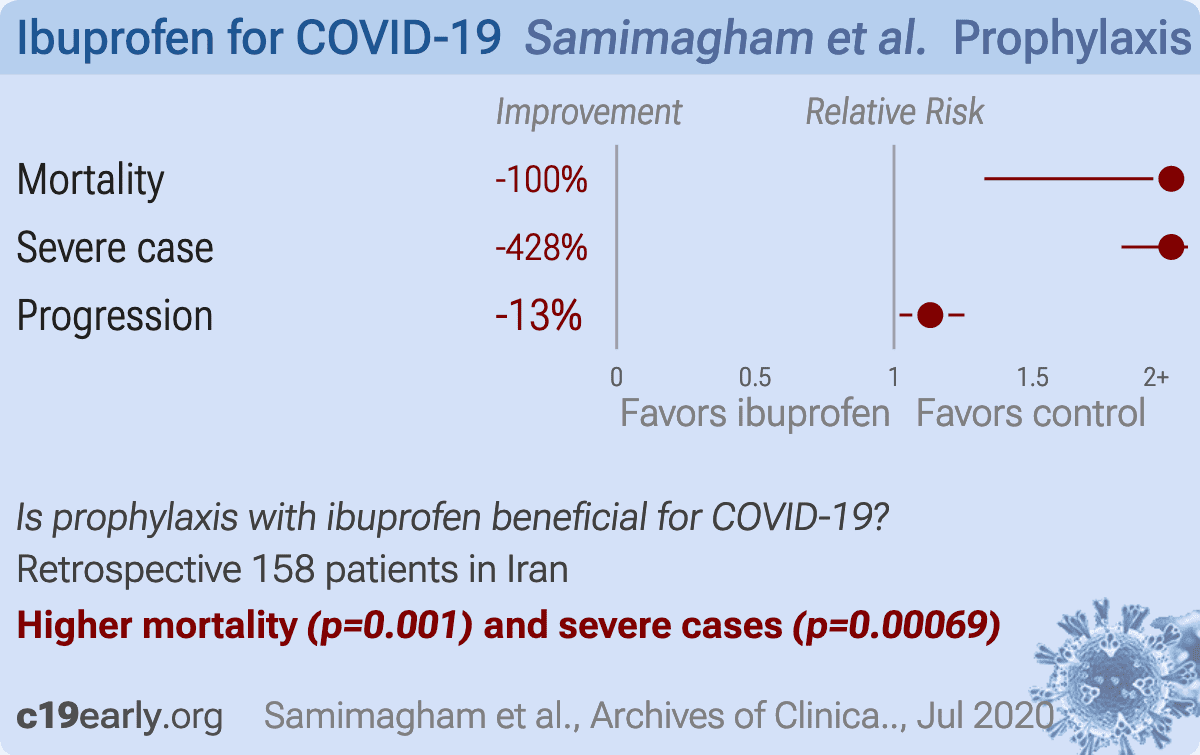
Retrospective 158 COVID-19 patients in Iran, showing higher risk of mortality with ibuprofen use.
{kind=link}
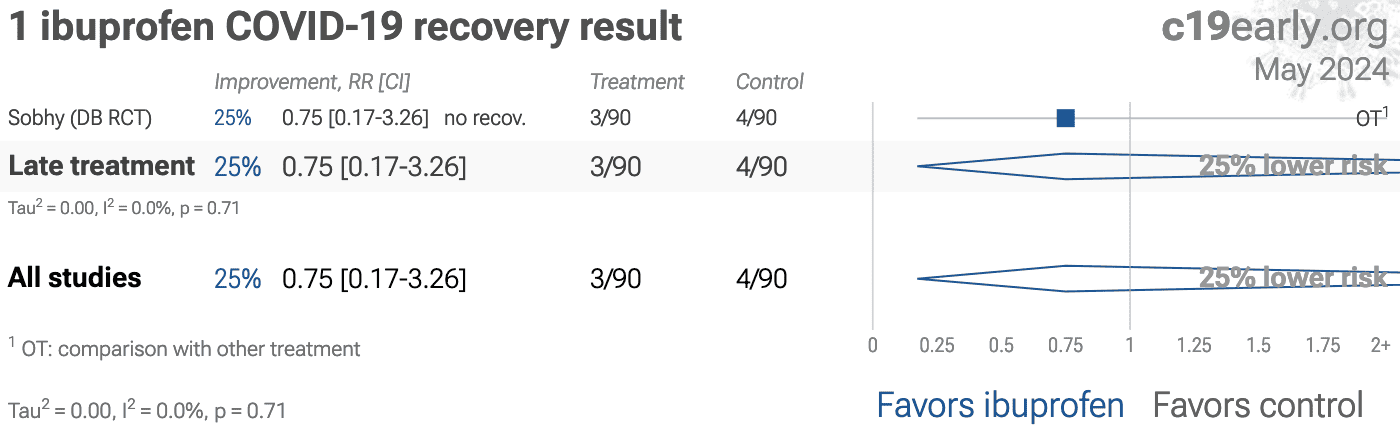
RCT 180 moderate hospitalized COVID-19 patients in Egypt, showing lower ICU admission and shorter hospitalization with ibuprofen compared with acetaminophen.
{kind=link}
Retrospective 2,463,707 people in the UK, showing no significant difference in COVID-19 mortality with NSAID use. Current NSAID users were defined as those ever prescribed an NSAID in the 4 months prior to study start, and non-users were those with no record of NSAID prescription in the same time period.
{kind=link}
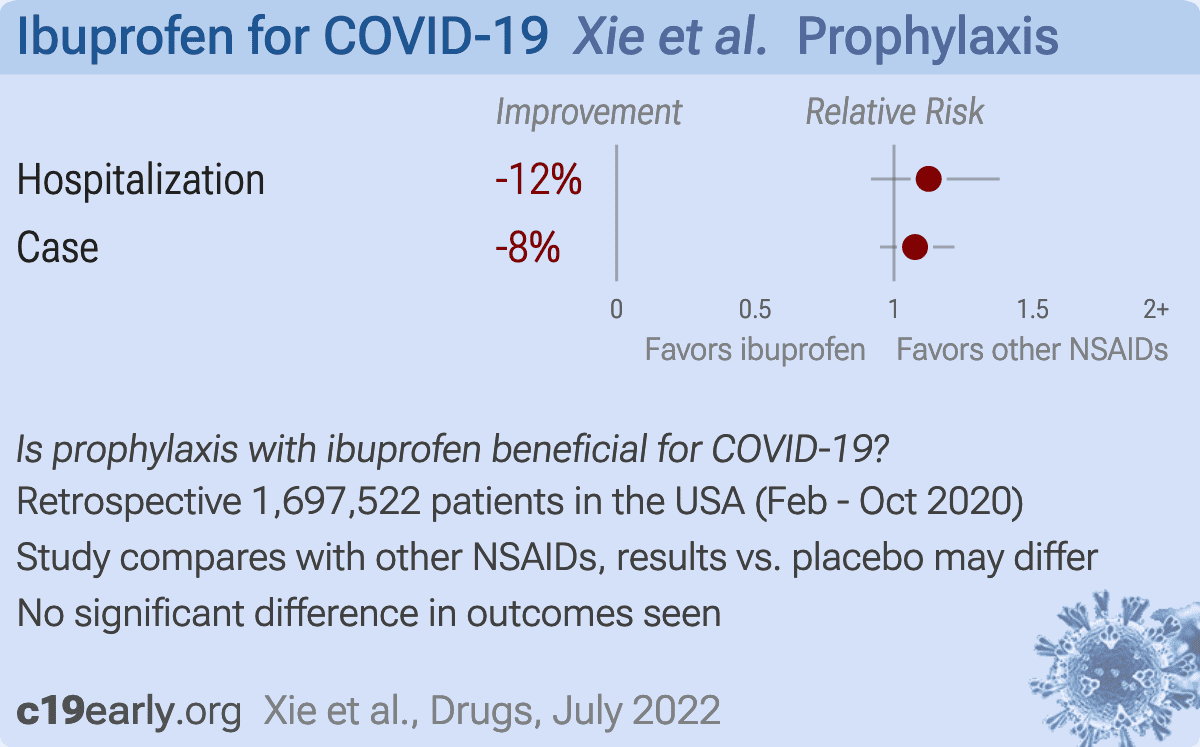
PSM retrospective 1,697,522 osteoarthritis or back pain patients in the US, showing no significant differences in COVID-19 cases and hospitalization for ibuprofen vs. other NSAIDs.
We perform ongoing searches of PubMed, medRxiv, Europe PMC,
ClinicalTrials.gov, The Cochrane Library, Google Scholar, Research
Square, ScienceDirect, Oxford University Press, the reference lists of other
studies and meta-analyses, and submissions to the site c19early.org.
Search terms are ibuprofen and COVID-19 or SARS-CoV-2. Automated searches are performed twice daily, with all matches reviewed for inclusion.
All studies regarding the use of ibuprofen for COVID-19 that report
a comparison with a control group are included in the main analysis.
Sensitivity analysis is performed, excluding studies with major issues,
epidemiological studies, and studies with minimal available information.
Studies with major unexplained data issues, for example major outcome data that
is impossible to be correct with no response from the authors, are excluded.
This is a living analysis and is updated regularly.
{kind=link}

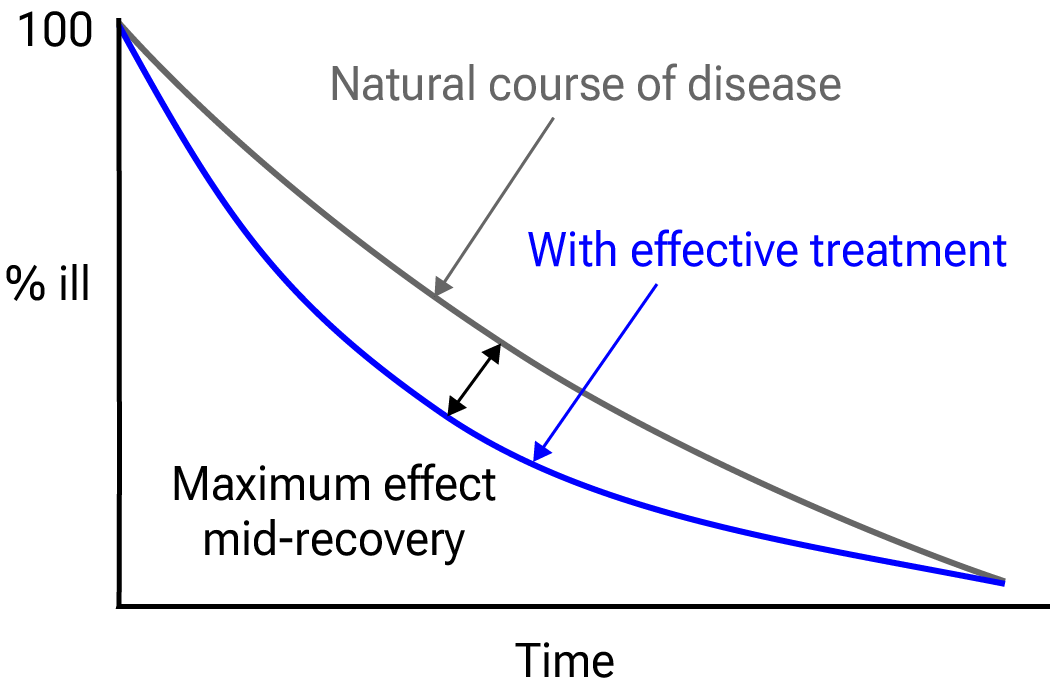
Figure 28.
Mid-recovery results can more accurately reflect efficacy when almost all patients
recover. Mateja et al. confirm that intermediate viral load results more accurately
reflect hospitalization/death.
We extracted effect sizes and associated data from all studies.
If studies report multiple kinds of effects then the most serious
outcome is used in pooled analysis, while other outcomes are included in the
outcome specific analyses. For example, if effects for mortality and cases are
reported then they are both used in specific outcome analyses, while mortality
is used for pooled analysis.
If symptomatic
results are reported at multiple times, we use the latest time, for example
if mortality results are provided at 14 days and 28 days, the results at 28
days have preference. Mortality alone is preferred over combined outcomes.
Outcomes with zero events in both arms are not used, the next most serious
outcome with one or more events is used. For example, in low-risk populations
with no mortality, a reduction in mortality with treatment is not possible,
however a reduction in hospitalization, for example, is still valuable.
Clinical outcomes are considered more important than viral outcomes.
When basically all patients recover in both treatment and control groups,
preference for viral clearance and recovery is given to results mid-recovery
where available. After most or all patients have recovered there is little or
no room for an effective treatment to do better, however faster recovery is
valuable.
An IPD meta-analysis confirms that intermediate viral load reduction
is more closely associated with hospitalization/death than later
viral load reduction134.
If only individual symptom data is available, the most serious symptom has
priority, for example difficulty breathing or low SpO2 is more
important than cough.
When results provide an odds ratio, we compute the relative risk when
possible, or convert to a relative risk according to Zhang et al.
Reported confidence intervals and p-values are used when available,
and adjusted values are used when provided. If multiple types of adjustments are
reported propensity score matching and multivariable regression has preference
over propensity score matching or weighting, which has preference over
multivariable regression. Adjusted results have preference over unadjusted
results for a more serious outcome when the adjustments significantly alter
results. When needed, conversion between reported p-values and
confidence intervals followed Altman, Altman (B), and Fisher's exact
test was used to calculate p-values for event data. If continuity
correction for zero values is required, we use the reciprocal of the opposite
arm with the sum of the correction factors equal to 1138.
Results are expressed with RR < 1.0 favoring treatment, and using the risk of
a negative outcome when applicable (for example, the risk of death rather than
the risk of survival). If studies only report relative continuous values such
as relative times, the ratio of the time for the treatment group versus the
time for the control group is used. Calculations are done in Python
(3.13.5) with
scipy (1.16.0), pythonmeta (1.26), numpy (2.3.1), statsmodels (0.14.4), and plotly (6.2.0).
Forest plots are computed using PythonMeta139
with the DerSimonian and Laird random effects model (the fixed effect
assumption is not plausible in this case) and inverse variance weighting.
Results are presented with 95% confidence intervals. Heterogeneity among studies was
assessed using the I2 statistic.
Mixed-effects meta-regression results are computed with R (4.4.0) using the metafor
(4.6-0) and rms (6.8-0) packages, and using the most serious sufficiently powered outcome.
For all statistical tests, a p-value less than 0.05 was considered statistically significant.
Grobid 0.8.2 is used to parse PDF documents.
We have classified studies as early treatment if most patients
are not already at a severe stage at the time of treatment (for example based
on oxygen status or lung involvement), and treatment started within 5 days of
the onset of symptoms. If studies contain a mix of early treatment and late
treatment patients, we consider the treatment time of patients contributing
most to the events (for example, consider a study where most patients are
treated early but late treatment patients are included, and all mortality
events were observed with late treatment patients).
We note that a shorter time may be preferable. Antivirals are typically only
considered effective when used within a shorter timeframe, for example 0-36 or
0-48 hours for oseltamivir, with longer delays not being effective57,58.
We received no funding, this research is done in our spare
time. We have no affiliations with any pharmaceutical companies or political
parties.
A summary of study results is below. Please submit
updates and corrections at https://c19early.org/ibmeta.html.
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
| Abu Esba, 11/2/2020, prospective, Saudi Arabia, peer-reviewed, 6 authors, study period 12 April, 2020 - 1 June, 2020, excluded in exclusion analyses: substantial unadjusted confounding by indication likely. | risk of death, 169.5% higher, RR 2.70, p = 0.35, treatment 1 of 40 (2.5%), control 11 of 357 (3.1%), adjusted per study, multivariable. |
| risk of death, 36.8% lower, HR 0.63, p = 0.68, treatment 40, control 357, Cox proportional hazards. | |
| risk of oxygen therapy, 44.8% higher, RR 1.45, p = 0.64, treatment 40, control 357, adjusted per study, multivariable. | |
| risk of hospitalization, 18.2% higher, RR 1.18, p = 0.64, treatment 40, control 357, adjusted per study, multivariable. | |
| risk of severe case, 84.8% higher, RR 1.85, p = 0.42, treatment 40, control 357, adjusted per study, multivariable. | |
| Rinott, 9/30/2020, retrospective, Israel, peer-reviewed, median age 45.0, 5 authors, study period 15 March, 2020 - 15 April, 2020. | risk of death, 21.1% higher, RR 1.21, p = 0.73, treatment 3 of 87 (3.4%), control 9 of 316 (2.8%). |
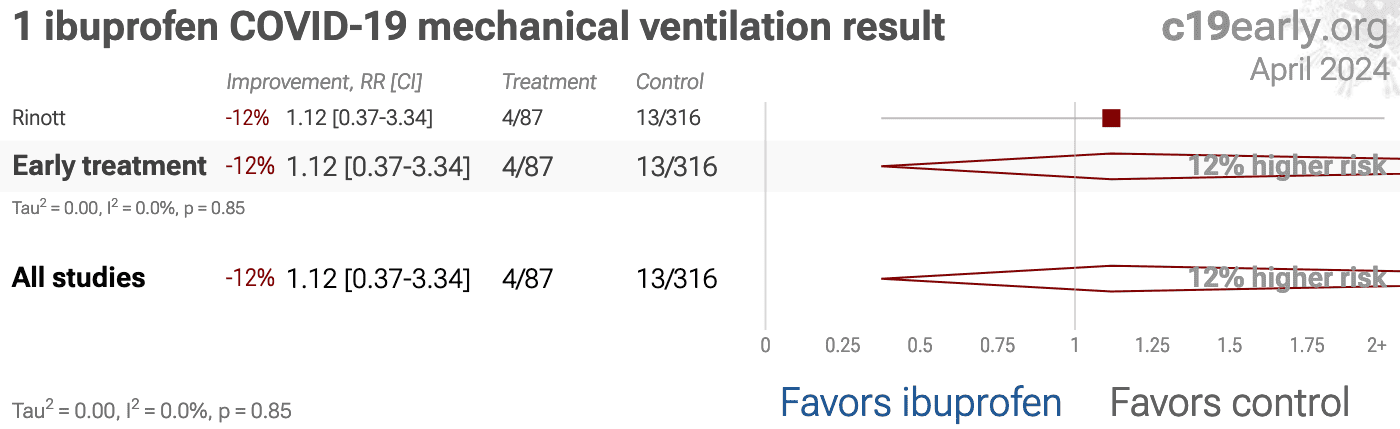
| risk of mechanical ventilation, 11.8% higher, RR 1.12, p = 0.77, treatment 4 of 87 (4.6%), control 13 of 316 (4.1%). | |
| risk of ICU admission, 39.7% higher, RR 1.40, p = 0.56, treatment 5 of 87 (5.7%), control 13 of 316 (4.1%). |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
| Sobhy, 4/19/2023, Double Blind Randomized Controlled Trial, Egypt, peer-reviewed, 6 authors, study period January 2022 - May 2022, this trial compares with another treatment - results may be better when compared to placebo, trial PACTR202202880140319. | risk of ICU admission, 52.4% lower, RR 0.48, p = 0.047, treatment 10 of 90 (11.1%), control 21 of 90 (23.3%), NNT 8.2. |
| risk of oxygen therapy, 52.4% lower, RR 0.48, p = 0.047, treatment 10 of 90 (11.1%), control 21 of 90 (23.3%), NNT 8.2. | |
| hospitalization time, 26.3% lower, relative time 0.74, p = 0.01, treatment 90, control 90. | |
| risk of no recovery, 25.0% lower, RR 0.75, p = 1.00, treatment 3 of 90 (3.3%), control 4 of 90 (4.4%), NNT 90, day 4, dyspnea. | |
| risk of no recovery, 42.9% lower, RR 0.57, p = 0.25, treatment 8 of 90 (8.9%), control 14 of 90 (15.6%), NNT 15, day 4, fever. | |
| risk of no recovery, 48.0% lower, RR 0.52, p = 0.04, treatment 13 of 90 (14.4%), control 25 of 90 (27.8%), NNT 7.5, day 4, lymphopenia. | |
| risk of no recovery, 41.2% lower, RR 0.59, p = 0.03, treatment 20 of 90 (22.2%), control 34 of 90 (37.8%), NNT 6.4, day 4, cough. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
| Campbell, 5/5/2022, retrospective, USA, peer-reviewed, 4 authors, study period 2 March, 2020 - 14 December, 2020. | risk of death, no change, OR 1.00, p = 0.54, treatment 1,814, control 20,311, adjusted per study, propensity score weighting, multivariable, day 60, RR approximated with OR. |
| risk of death, 1.0% lower, OR 0.99, p = 0.23, treatment 1,814, control 20,311, adjusted per study, propensity score weighting, multivariable, day 30, RR approximated with OR. | |
| Choi, 6/23/2020, retrospective, South Korea, peer-reviewed, median age 29.0, 8 authors, study period 5 March, 2020 - 18 March, 2020. | risk of progression, 240.0% higher, OR 3.40, p = 0.26, treatment 6 of 36 (16.7%) cases, 2 of 36 (5.6%) controls, case control OR, propensity score matching. |
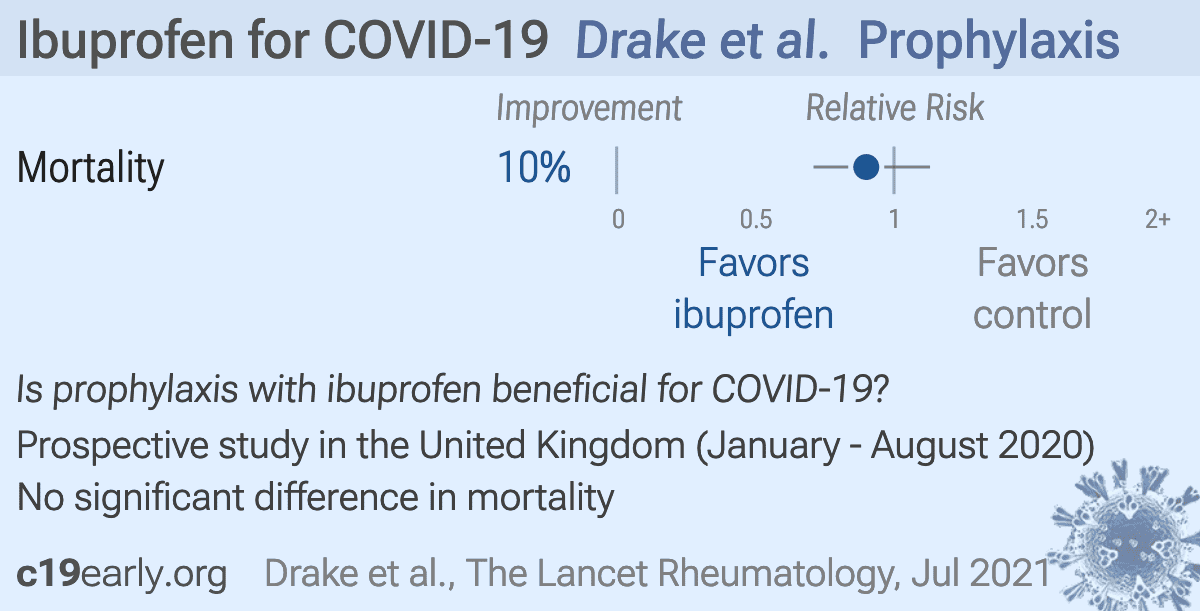
| Drake, 7/31/2021, prospective, United Kingdom, peer-reviewed, 13 authors, study period 17 January, 2020 - 10 August, 2020. | risk of death, 10.0% lower, OR 0.90, p = 0.36, adjusted per study, multivariable, RR approximated with OR. |
| Kragholm, 10/21/2020, retrospective, Denmark, peer-reviewed, 13 authors, study period 1 January, 2020 - 30 April, 2020. | risk of progression, 4.0% lower, RR 0.96, p = 0.78, treatment 264, control 3,738. |
| Leal, 8/16/2021, retrospective, United Kingdom, peer-reviewed, 5 authors, study period 16 March, 2020 - 1 February, 2021. | risk of case, 3.0% lower, OR 0.97, p = 0.29, RR approximated with OR. |
| Loucera, 8/16/2022, retrospective, Spain, peer-reviewed, 8 authors, study period January 2020 - November 2020. | risk of death, 48.3% lower, HR 0.52, p = 0.002, treatment 519, control 15,449, Cox proportional hazards, day 30. |
| Reese, 4/20/2021, retrospective, USA, preprint, 23 authors. | risk of death, 9.0% lower, HR 0.91, p = 0.65, treatment 5,737, control 5,737, propensity score matching, Cox proportional hazards, Table S56. |
| risk of severe case, 303.0% higher, OR 4.03, p < 0.001, treatment 5,737, control 5,737, propensity score matching, Table S48, RR approximated with OR. | |
| Samimagham, 7/13/2020, retrospective, Iran, peer-reviewed, 4 authors. | risk of death, 100% higher, OR 2.00, p < 0.001, treatment 63, control 95, adjusted per study, multivariable, RR approximated with OR. |
| risk of severe case, 427.8% higher, RR 5.28, p < 0.001, treatment 14 of 63 (22.2%), control 4 of 95 (4.2%). | |
| risk of progression, 13.1% higher, RR 1.13, p = 0.04, treatment 60 of 63 (95.2%), control 80 of 95 (84.2%), moderate or severe. | |
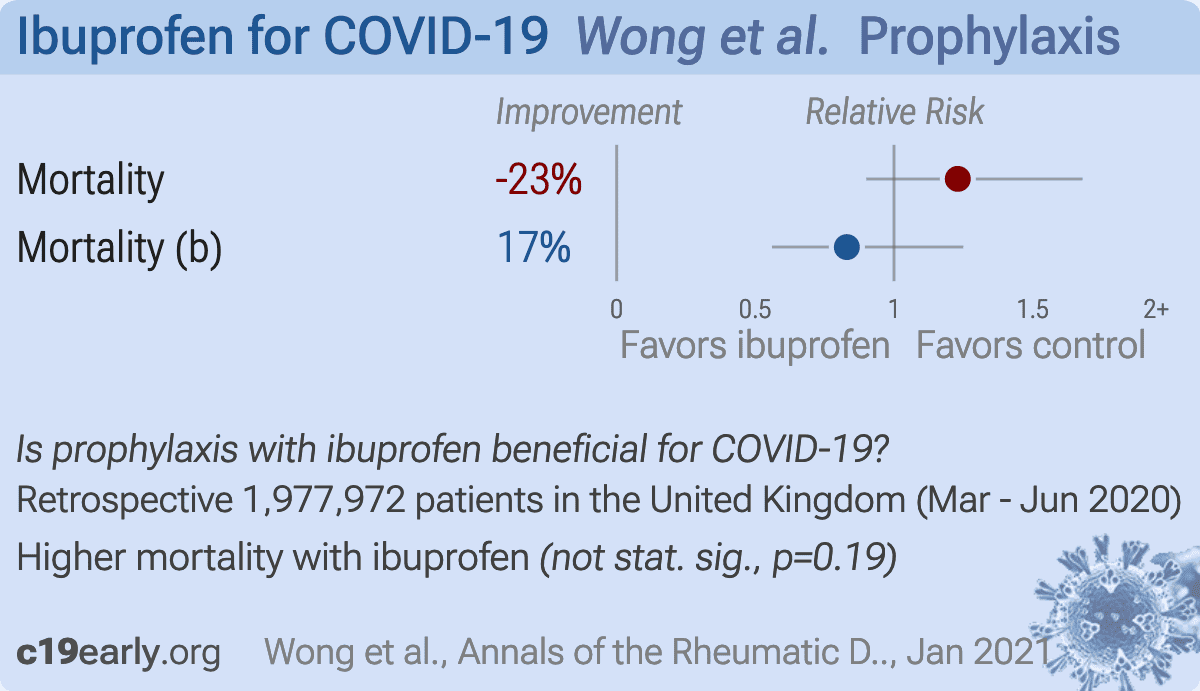
| Wong, 1/21/2021, retrospective, United Kingdom, peer-reviewed, median age 53.0, 32 authors, study period 1 March, 2020 - 14 June, 2020. | risk of death, 23.0% higher, HR 1.23, p = 0.19, adjusted per study, general population, multivariable. |
| risk of death, 17.0% lower, HR 0.83, p = 0.37, adjusted per study, rheumatoid arthritis/osteoarthritis patients, multivariable. | |
| Xie (B), 7/13/2022, retrospective, USA, peer-reviewed, 9 authors, study period 1 February, 2020 - 31 October, 2020, this trial compares with another treatment - results may be better when compared to placebo. | risk of hospitalization, 12.5% higher, HR 1.12, p = 0.26, Open Claims, PharMetrics Plus, both periods combined. |
| risk of case, 7.6% higher, HR 1.08, p = 0.25, Open Claims, PharMetrics Plus, both periods combined. |
Viral infection and replication involves attachment, entry, uncoating and release, genome replication and transcription, translation and protein processing, assembly and budding, and release. Each step can be disrupted by therapeutics.
Day, M., Covid-19: ibuprofen should not be used for managing symptoms, say doctors and scientists, BMJ, doi:10.1136/bmj.m1086.
Ryu et al., Fibrin drives thromboinflammation and neuropathology in COVID-19, Nature, doi:10.1038/s41586-024-07873-4.
Rong et al., Persistence of spike protein at the skull-meninges-brain axis may contribute to the neurological sequelae of COVID-19, Cell Host & Microbe, doi:10.1016/j.chom.2024.11.007.
Yang et al., SARS-CoV-2 infection causes dopaminergic neuron senescence, Cell Stem Cell, doi:10.1016/j.stem.2023.12.012.
Scardua-Silva et al., Microstructural brain abnormalities, fatigue, and cognitive dysfunction after mild COVID-19, Scientific Reports, doi:10.1038/s41598-024-52005-7.
Hampshire et al., Cognition and Memory after Covid-19 in a Large Community Sample, New England Journal of Medicine, doi:10.1056/NEJMoa2311330.
Duloquin et al., Is COVID-19 Infection a Multiorganic Disease? Focus on Extrapulmonary Involvement of SARS-CoV-2, Journal of Clinical Medicine, doi:10.3390/jcm13051397.
Sodagar et al., Pathological Features and Neuroinflammatory Mechanisms of SARS-CoV-2 in the Brain and Potential Therapeutic Approaches, Biomolecules, doi:10.3390/biom12070971.
Sagar et al., COVID-19-associated cerebral microbleeds in the general population, Brain Communications, doi:10.1093/braincomms/fcae127.
Verma et al., Persistent Neurological Deficits in Mouse PASC Reveal Antiviral Drug Limitations, bioRxiv, doi:10.1101/2024.06.02.596989.
Panagea et al., Neurocognitive Impairment in Long COVID: A Systematic Review, Archives of Clinical Neuropsychology, doi:10.1093/arclin/acae042.
Ariza et al., COVID-19: Unveiling the Neuropsychiatric Maze—From Acute to Long-Term Manifestations, Biomedicines, doi:10.3390/biomedicines12061147.
Vashisht et al., Neurological Complications of COVID-19: Unraveling the Pathophysiological Underpinnings and Therapeutic Implications, Viruses, doi:10.3390/v16081183.
Ahmad et al., Neurological Complications and Outcomes in Critically Ill Patients With COVID-19: Results From International Neurological Study Group From the COVID-19 Critical Care Consortium, The Neurohospitalist, doi:10.1177/19418744241292487.
Wang et al., SARS-CoV-2 membrane protein induces neurodegeneration via affecting Golgi-mitochondria interaction, Translational Neurodegeneration, doi:10.1186/s40035-024-00458-1.
Eberhardt et al., SARS-CoV-2 infection triggers pro-atherogenic inflammatory responses in human coronary vessels, Nature Cardiovascular Research, doi:10.1038/s44161-023-00336-5.
Van Tin et al., Spike Protein of SARS-CoV-2 Activates Cardiac Fibrogenesis through NLRP3 Inflammasomes and NF-κB Signaling, Cells, doi:10.3390/cells13161331.
Borka Balas et al., COVID-19 and Cardiac Implications—Still a Mystery in Clinical Practice, Reviews in Cardiovascular Medicine, doi:10.31083/j.rcm2405125.
AlTaweel et al., An In-Depth Insight into Clinical, Cellular and Molecular Factors in COVID19-Associated Cardiovascular Ailments for Identifying Novel Disease Biomarkers, Drug Targets and Clinical Management Strategies, Archives of Microbiology & Immunology, doi:10.26502/ami.936500177.
Saha et al., COVID-19 beyond the lungs: Unraveling its vascular impact and cardiovascular complications—mechanisms and therapeutic implications, Science Progress, doi:10.1177/00368504251322069.
Trender et al., Changes in memory and cognition during the SARS-CoV-2 human challenge study, eClinicalMedicine, doi:10.1016/j.eclinm.2024.102842.
Dugied et al., Multimodal SARS-CoV-2 interactome sketches the virus-host spatial organization, Communications Biology, doi:10.1038/s42003-025-07933-z.
Malone et al., Structures and functions of coronavirus replication–transcription complexes and their relevance for SARS-CoV-2 drug design, Nature Reviews Molecular Cell Biology, doi:10.1038/s41580-021-00432-z.
Murigneux et al., Proteomic analysis of SARS-CoV-2 particles unveils a key role of G3BP proteins in viral assembly, Nature Communications, doi:10.1038/s41467-024-44958-0.
Lv et al., Host proviral and antiviral factors for SARS-CoV-2, Virus Genes, doi:10.1007/s11262-021-01869-2.
Lui et al., Nsp1 facilitates SARS-CoV-2 replication through calcineurin-NFAT signaling, Virology, doi:10.1128/mbio.00392-24.
Niarakis et al., Drug-target identification in COVID-19 disease mechanisms using computational systems biology approaches, Frontiers in Immunology, doi:10.3389/fimmu.2023.1282859.
Katiyar et al., SARS-CoV-2 Assembly: Gaining Infectivity and Beyond, Viruses, doi:10.3390/v16111648.
Wu et al., Decoding the genome of SARS-CoV-2: a pathway to drug development through translation inhibition, RNA Biology, doi:10.1080/15476286.2024.2433830.
Stuart et al., NSAID prescribing and adverse outcomes in common infections: a population-based cohort study, BMJ Open, doi:10.1136/bmjopen-2023-077365.
Wrotek et al., Let fever do its job, Evolution, Medicine, and Public Health, doi:10.1093/emph/eoaa044.
Evans et al., Fever and the thermal regulation of immunity: the immune system feels the heat, Nature Reviews Immunology, doi:10.1038/nri3843.
Los et al., Body temperature variation controls pre-mRNA processing and transcription of antiviral genes and SARS-CoV-2 replication, Nucleic Acids Research, doi:10.1093/nar/gkac513.
Zhou et al., Temperature dependence of the SARS-CoV-2 affinity to human ACE2 determines COVID-19 progression and clinical outcome, Computational and Structural Biotechnology Journal, doi:10.1016/j.csbj.2020.12.005.
Downing et al., Hyperthermia in Humans Enhances Interferon-γ Synthesis and Alters the Peripheral Lymphocyte Population, Journal of Interferon Research, doi:10.1089/jir.1988.8.143.
Herder et al., Elevated temperature inhibits SARS-CoV-2 replication in respiratory epithelium independently of IFN-mediated innate immune defenses, PLOS Biology, doi:10.1371/journal.pbio.3001065.
Dominguez-Nicolas et al., Low-field thoracic magnetic stimulation increases peripheral oxygen saturation levels in coronavirus disease (COVID-19) patients, Medicine, doi:10.1097/MD.0000000000027444.
Ramirez et al., Hydrothermotherapy in prevention and treatment of mild to moderate cases of COVID-19, Medical Hypotheses, doi:10.1016/j.mehy.2020.110363.
Ruble, W., Sanitarium Treatment of Influenza Life and Health, May 1919, 34:5, documents.adventistarchives.org/Periodicals/LH/LH19190501-V34-05.pdf.
Stewart, H., Diathermy in the Treatment of Pneumonia, Proceedings of the Royal Society of Medicine, 19:53-56, www.ncbi.nlm.nih.gov/pmc/articles/PMC1948555/.
Xie et al., Molecular Basis of High-Blood-Pressure-Enhanced and High-Fever-Temperature-Weakened Receptor-Binding Domain/Peptidase Domain Binding: A Molecular Dynamics Simulation Study, International Journal of Molecular Sciences, doi:10.3390/ijms26073250.
Zeraatkar et al., Consistency of covid-19 trial preprints with published reports and impact for decision making: retrospective review, BMJ Medicine, doi:10.1136/bmjmed-2022-0003091.
Davidson et al., No evidence of important difference in summary treatment effects between COVID-19 preprints and peer-reviewed publications: a meta-epidemiological study, Journal of Clinical Epidemiology, doi:10.1016/j.jclinepi.2023.08.011.
Jadad et al., Randomized Controlled Trials: Questions, Answers, and Musings, Second Edition, doi:10.1002/9780470691922.
Gøtzsche, P., Bias in double-blind trials, Doctoral Thesis, University of Copenhagen, www.scientificfreedom.dk/2023/05/16/bias-in-double-blind-trials-doctoral-thesis/.
Als-Nielsen et al., Association of Funding and Conclusions in Randomized Drug Trials, JAMA, doi:10.1001/jama.290.7.921.
Anglemyer et al., Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials, Cochrane Database of Systematic Reviews 2014, Issue 4, doi:10.1002/14651858.MR000034.pub2.
Lee et al., Analysis of Overall Level of Evidence Behind Infectious Diseases Society of America Practice Guidelines, Arch Intern Med., 2011, 171:1, 18-22, doi:10.1001/archinternmed.2010.482.
Deaton et al., Understanding and misunderstanding randomized controlled trials, Social Science & Medicine, 210, doi:10.1016/j.socscimed.2017.12.005.
Nichol et al., Challenging issues in randomised controlled trials, Injury, 2010, doi: 10.1016/j.injury.2010.03.033, www.injuryjournal.com/article/S0020-1383(10)00233-0/fulltext.
Abu Esba et al., Ibuprofen and NSAID Use in COVID-19 Infected Patients Is Not Associated with Worse Outcomes: A Prospective Cohort Study, Infectious Diseases and Therapy, doi:10.1007/s40121-020-00363-w.
Treanor et al., Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza: A Randomized Controlled Trial, JAMA, 2000, 283:8, 1016-1024, doi:10.1001/jama.283.8.1016.
McLean et al., Impact of Late Oseltamivir Treatment on Influenza Symptoms in the Outpatient Setting: Results of a Randomized Trial, Open Forum Infect. Dis. September 2015, 2:3, doi:10.1093/ofid/ofv100.
Ikematsu et al., Baloxavir Marboxil for Prophylaxis against Influenza in Household Contacts, New England Journal of Medicine, doi:10.1056/NEJMoa1915341.
Hayden et al., Baloxavir Marboxil for Uncomplicated Influenza in Adults and Adolescents, New England Journal of Medicine, doi:10.1056/NEJMoa1716197.
Kumar et al., Combining baloxavir marboxil with standard-of-care neuraminidase inhibitor in patients hospitalised with severe influenza (FLAGSTONE): a randomised, parallel-group, double-blind, placebo-controlled, superiority trial, The Lancet Infectious Diseases, doi:10.1016/S1473-3099(21)00469-2.
López-Medina et al., Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2021.3071.
Korves et al., SARS-CoV-2 Genetic Variants and Patient Factors Associated with Hospitalization Risk, medRxiv, doi:10.1101/2024.03.08.24303818.
Faria et al., Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil, Science, doi:10.1126/science.abh2644.
Nonaka et al., SARS-CoV-2 variant of concern P.1 (Gamma) infection in young and middle-aged patients admitted to the intensive care units of a single hospital in Salvador, Northeast Brazil, February 2021, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.08.003.
Karita et al., Trajectory of viral load in a prospective population-based cohort with incident SARS-CoV-2 G614 infection, medRxiv, doi:10.1101/2021.08.27.21262754.
Zavascki et al., Advanced ventilatory support and mortality in hospitalized patients with COVID-19 caused by Gamma (P.1) variant of concern compared to other lineages: cohort study at a reference center in Brazil, Research Square, doi:10.21203/rs.3.rs-910467/v1.
Willett et al., The hyper-transmissible SARS-CoV-2 Omicron variant exhibits significant antigenic change, vaccine escape and a switch in cell entry mechanism, medRxiv, doi:10.1101/2022.01.03.21268111.
Peacock et al., The SARS-CoV-2 variant, Omicron, shows rapid replication in human primary nasal epithelial cultures and efficiently uses the endosomal route of entry, bioRxiv, doi:10.1101/2021.12.31.474653.
Williams, T., Not All Ivermectin Is Created Equal: Comparing The Quality of 11 Different Ivermectin Sources, Do Your Own Research, doyourownresearch.substack.com/p/not-all-ivermectin-is-created-equal.
Xu et al., A study of impurities in the repurposed COVID-19 drug hydroxychloroquine sulfate by UHPLC-Q/TOF-MS and LC-SPE-NMR, Rapid Communications in Mass Spectrometry, doi:10.1002/rcm.9358.
Jitobaom et al., Favipiravir and Ivermectin Showed in Vitro Synergistic Antiviral Activity against SARS-CoV-2, Research Square, doi:10.21203/rs.3.rs-941811/v1.
Jitobaom (B) et al., Synergistic anti-SARS-CoV-2 activity of repurposed anti-parasitic drug combinations, BMC Pharmacology and Toxicology, doi:10.1186/s40360-022-00580-8.
Jeffreys et al., Remdesivir-ivermectin combination displays synergistic interaction with improved in vitro activity against SARS-CoV-2, International Journal of Antimicrobial Agents, doi:10.1016/j.ijantimicag.2022.106542.
Ostrov et al., Highly Specific Sigma Receptor Ligands Exhibit Anti-Viral Properties in SARS-CoV-2 Infected Cells, Pathogens, doi:10.3390/pathogens10111514.
Alsaidi et al., Griffithsin and Carrageenan Combination Results in Antiviral Synergy against SARS-CoV-1 and 2 in a Pseudoviral Model, Marine Drugs, doi:10.3390/md19080418.
Andreani et al., In vitro testing of combined hydroxychloroquine and azithromycin on SARS-CoV-2 shows synergistic effect, Microbial Pathogenesis, doi:10.1016/j.micpath.2020.104228.
De Forni et al., Synergistic drug combinations designed to fully suppress SARS-CoV-2 in the lung of COVID-19 patients, PLoS ONE, doi:10.1371/journal.pone.0276751.
Wan et al., Synergistic inhibition effects of andrographolide and baicalin on coronavirus mechanisms by downregulation of ACE2 protein level, Scientific Reports, doi:10.1038/s41598-024-54722-5.
Said et al., The effect of Nigella sativa and vitamin D3 supplementation on the clinical outcome in COVID-19 patients: A randomized controlled clinical trial, Frontiers in Pharmacology, doi:10.3389/fphar.2022.1011522.
Fiaschi et al., In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants, Viruses, doi:10.3390/v16020168.
Xing et al., Published anti-SARS-CoV-2 in vitro hits share common mechanisms of action that synergize with antivirals, Briefings in Bioinformatics, doi:10.1093/bib/bbab249.
Chen et al., Synergistic Inhibition of SARS-CoV-2 Replication Using Disulfiram/Ebselen and Remdesivir, ACS Pharmacology & Translational Science, doi:10.1021/acsptsci.1c00022.
Hempel et al., Synergistic inhibition of SARS-CoV-2 cell entry by otamixaban and covalent protease inhibitors: pre-clinical assessment of pharmacological and molecular properties, Chemical Science, doi:10.1039/D1SC01494C.
Schultz et al., Pyrimidine inhibitors synergize with nucleoside analogues to block SARS-CoV-2, Nature, doi:10.1038/s41586-022-04482-x.
Ohashi et al., Potential anti-COVID-19 agents, cepharanthine and nelfinavir, and their usage for combination treatment, iScience, doi:10.1016/j.isci.2021.102367.
Al Krad et al., The protease inhibitor Nirmatrelvir synergizes with inhibitors of GRP78 to suppress SARS-CoV-2 replication, bioRxiv, doi:10.1101/2025.03.09.642200.
Thairu et al., A Comparison of Ivermectin and Non Ivermectin Based Regimen for COVID-19 in Abuja: Effects on Virus Clearance, Days-to-discharge and Mortality, Journal of Pharmaceutical Research International, doi:10.9734/jpri/2022/v34i44A36328.
Singh et al., The relationship between viral clearance rates and disease progression in early symptomatic COVID-19: a systematic review and meta-regression analysis, Journal of Antimicrobial Chemotherapy, doi:10.1093/jac/dkae045.
Boulware, D., Comments regarding paper rejection, twitter.com/boulware_dr/status/1311331372884205570.
Rothstein, H., Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments, www.wiley.com/en-ae/Publication+Bias+in+Meta+Analysis:+Prevention,+Assessment+and+Adjustments-p-9780470870143.
Stanley et al., Meta-regression approximations to reduce publication selection bias, Research Synthesis Methods, doi:10.1002/jrsm.1095.
Rücker et al., Arcsine test for publication bias in meta-analyses with binary outcomes, Statistics in Medicine, doi:10.1002/sim.2971.
Peters, J., Comparison of Two Methods to Detect Publication Bias in Meta-analysis, JAMA, doi:10.1001/jama.295.6.676.
Moreno et al., Assessment of regression-based methods to adjust for publication bias through a comprehensive simulation study, BMC Medical Research Methodology, doi:10.1186/1471-2288-9-2.
Macaskill et al., A comparison of methods to detect publication bias in meta-analysis, Statistics in Medicine, doi:10.1002/sim.698.
Egger et al., Bias in meta-analysis detected by a simple, graphical test, BMJ, doi:10.1136/bmj.315.7109.629.
Harbord et al., A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints, Statistics in Medicine, doi:10.1002/sim.2380.
Moshawih et al., Evaluating NSAIDs in SARS-CoV-2: Immunomodulatory mechanisms and future therapeutic strategies, Heliyon, doi:10.1016/j.heliyon.2024.e25734.
Zurita-Lizza et al., Repurposing Inhaled Ibuprofenate, a Non Steroidal Anti‐Inflammatory Drug, as a Potential Adjuvant Treatment for Pneumonia, CARDS and its Aetiological Agent SARS‐CoV‐2, Clinical and Translational Discovery, doi:10.1002/ctd2.204.
Rinott et al., Ibuprofen use and clinical outcomes in COVID-19 patients, Clinical Microbiology and Infection, doi:10.1016/j.cmi.2020.06.003.
Sobhy et al., Early Use of Ibuprofen in Moderate Cases of COVID-19 Might be a Promising Agent to Attenuate the Severity of Disease: A Randomized Controlled Trial, The Open Anesthesia Journal, doi:10.2174/25896458-v17-e230403-2022-26.
Kalayan et al., Safety and Efficacy of Nebulised Anti-Inflammatory Solution of Alkaline Hypertonic Ibuprofen (AHI) for Treatment of SARS-Cov-2 Infection: A Compassionate Study with a Comparator Arms, European Journal of Respiratory Medicine, doi:10.31488/EJRM.132.
Calonico et al., Causal Inference During a Pandemic: Evidence on the Effectiveness of Nebulized Ibuprofen as an Unproven Treatment for COVID-19 in Argentina, National Bureau of Economic Research, doi:10.3386/w30084.
Salva et al., Reversal of SARS-CoV2-Induced Hypoxia by Nebulized Sodium Ibuprofenate in a Compassionate Use Program, Infectious Diseases and Therapy, doi:10.1007/s40121-021-00527-2.
Loucera et al., Real-world evidence with a retrospective cohort of 15,968 COVID-19 hospitalized patients suggests 21 new effective treatments, Virology Journal, doi:10.1186/s12985-023-02195-9.
Xie (B) et al., Risk of COVID-19 Diagnosis and Hospitalization in Patients with Osteoarthritis or Back Pain Treated with Ibuprofen Compared to Other NSAIDs or Paracetamol: A Network Cohort Study, Drugs, doi:10.1007/s40265-022-01822-z.
Campbell et al., Chronic use of non-steroidal anti-inflammatory drugs (NSAIDs) or acetaminophen and relationship with mortality among United States Veterans after testing positive for COVID-19, PLOS ONE, doi:10.1371/journal.pone.0267462.
Leal et al., Paracetamol Is Associated with a Lower Risk of COVID-19 Infection and Decreased ACE2 Protein Expression: A Retrospective Analysis, COVID, doi:10.3390/covid1010018.
Drake et al., Non-steroidal anti-inflammatory drug use and outcomes of COVID-19 in the ISARIC Clinical Characterisation Protocol UK cohort: a matched, prospective cohort study, The Lancet Rheumatology, doi:10.1016/S2665-9913(21)00104-1.
Reese et al., Cyclooxygenase inhibitor use is associated with increased COVID-19 severity, medRxiv, doi:10.1101/2021.04.13.21255438.
Wong et al., Use of non-steroidal anti-inflammatory drugs and risk of death from COVID-19: an OpenSAFELY cohort analysis based on two cohorts, Annals of the Rheumatic Diseases, doi:10.1136/annrheumdis-2020-219517.
Kragholm et al., Association Between Prescribed Ibuprofen and Severe COVID-19 Infection: A Nationwide Register-Based Cohort Study, Clinical and Translational Science, doi:10.1111/cts.12904.
Samimagham et al., The Association of Non-Steroidal Anti-Inflammatory Drugs with COVID-19 Severity and Mortality, Archives of Clinical Infectious Diseases, doi:10.5812/archcid.106847.
Choi et al., Clinical Characteristics and Disease Progression in Early-Stage COVID-19 Patients in South Korea, Journal of Clinical Medicine, doi:10.3390/jcm9061959.
Hanai, T., COVID-19, Infection Inhibitors and Medicines, MDPI AG, doi:10.20944/preprints202501.1042.v1.
Paranga et al., Cytokine Storm in COVID-19: Exploring IL-6 Signaling and Cytokine-Microbiome Interactions as Emerging Therapeutic Approaches, International Journal of Molecular Sciences, doi:10.3390/ijms252111411.
Alzahrani, K., Repurposing of Anti-Cancer Drugs Against Moderate and Severe COVID Infection: A Network-Based Systems Biological Approach, Nigerian Journal of Clinical Practice, doi:10.4103/njcp.njcp_873_23.
Girgis et al., Indole-based compounds as potential drug candidates for SARS-CoV-2, MDPI AG, doi:10.20944/preprints202308.0746.v1.
Loucera (B) et al., Drug repurposing for COVID-19 using machine learning and mechanistic models of signal transduction circuits related to SARS-CoV-2 infection, Signal Transduction and Targeted Therapy, doi:10.1038/s41392-020-00417-y.
Kushwaha et al., A comprehensive review on the global efforts on vaccines and repurposed drugs for combating COVID-19, European Journal of Medicinal Chemistry, doi:10.1016/j.ejmech.2023.115719.
Oliver et al., Different drug approaches to COVID-19 treatment worldwide: an update of new drugs and drugs repositioning to fight against the novel coronavirus, Therapeutic Advances in Vaccines and Immunotherapy, doi:10.1177/25151355221144845.
Kumar (B) et al., COVID-19 therapeutics: Clinical application of repurposed drugs and futuristic strategies for target-based drug discovery, Genes & Diseases, doi:10.1016/j.gendis.2022.12.019.
Homolak et al., Widely available lysosome targeting agents should be considered as potential therapy for COVID-19, International Journal of Antimicrobial Agents, doi:10.1016/j.ijantimicag.2020.106044.
Mostafa et al., FDA-Approved Drugs with Potent In Vitro Antiviral Activity against Severe Acute Respiratory Syndrome Coronavirus 2, Pharmaceuticals, doi:10.3390/ph13120443.
Supianto et al., Cluster-based text mining for extracting drug candidates for the prevention of COVID-19 from the biomedical literature, Journal of Taibah University Medical Sciences, doi:10.1016/j.jtumed.2022.12.015.
Sperry et al., Target-agnostic drug prediction integrated with medical record analysis uncovers differential associations of statins with increased survival in COVID-19 patients, PLOS Computational Biology, doi:10.1371/journal.pcbi.1011050.
Issac et al., Improved And Optimized Drug Repurposing For The SARS-CoV-2 Pandemic, bioRxiv, doi:10.1101/2022.03.24.485618.
Sarkar et al., Potential Therapeutic Options for COVID-19: Current Status, Challenges, and Future Perspectives, Frontiers in Pharmacology, doi:10.3389/fphar.2020.572870.
Mateja et al., The choice of viral load endpoint in early phase trials of COVID-19 treatments aiming to reduce 28-day hospitalization and/or death, The Journal of Infectious Diseases, doi:10.1093/infdis/jiaf282.
Zhang et al., What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes, JAMA, 80:19, 1690, doi:10.1001/jama.280.19.1690.
Altman (B) et al., How to obtain the confidence interval from a P value, BMJ, doi:10.1136/bmj.d2090.
Please send us corrections, updates, or comments.
c19early involves the extraction of 200,000+ datapoints from
thousands of papers. Community updates
help ensure high accuracy.
Treatments and other interventions are complementary.
All practical, effective, and safe
means should be used based on risk/benefit analysis.
No treatment or intervention is 100% available and effective for all current
and future variants.
We do not provide medical advice. Before taking any medication,
consult a qualified physician who can provide personalized advice and details
of risks and benefits based on your medical history and situation. IMA and WCH
provide treatment protocols.